What Is the ICD-10 Code for Mixed Hyperlipidemia?
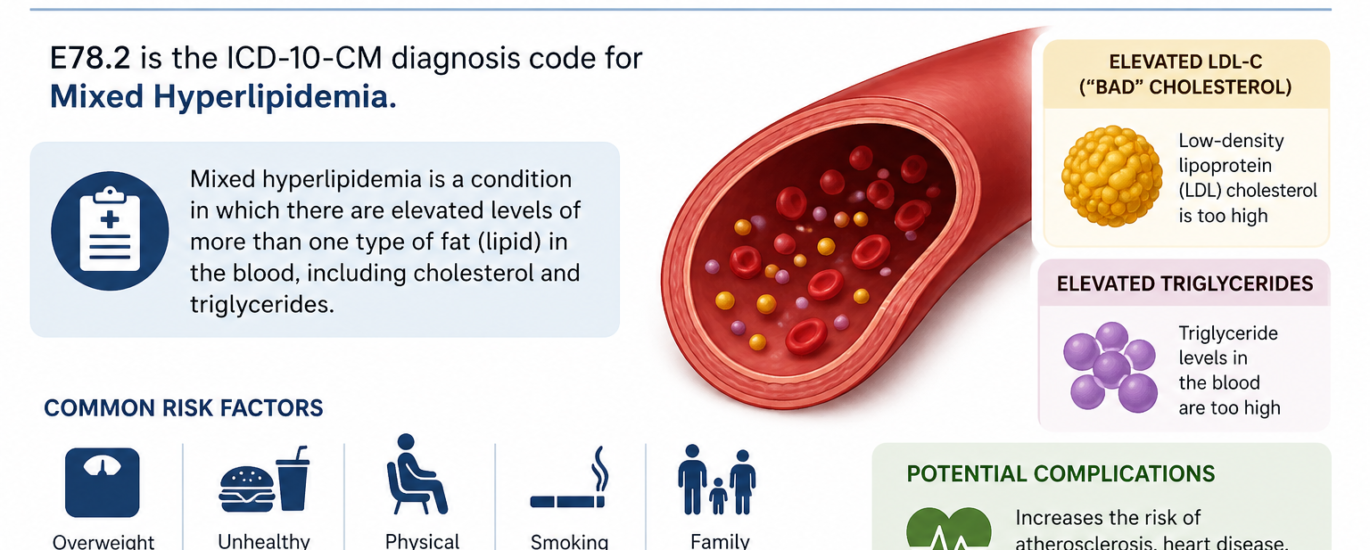
If you work as a medical coder, biller, or healthcare provider, you probably handle lipid disorder codes every single day. So let’s cut straight to the answer: the ICD-10 code for mixed hyperlipidemia is E78.2. Physicians and coders use this billable, highly specific ICD-10-CM code to document and bill for a condition where a patient carries both elevated cholesterol and elevated triglycerides at the same time.
This code falls under Chapter 4 of the ICD-10-CM system, which covers endocrine, nutritional, and metabolic diseases. More specifically, E78.2 sits within the E78 category, which groups all disorders of lipoprotein metabolism and other lipidemias together. The 2026 edition of this code took effect on October 1, 2025, and it remains valid for HIPAA-covered claims through September 30, 2026.
Understanding this code goes far beyond a billing formality. It directly shapes reimbursement outcomes, claim approval rates, audit results, and most importantly, the quality of your patient care documentation.
What Exactly Is Mixed Hyperlipidemia?
Before diving into the coding specifics, it helps to understand what mixed hyperlipidemia actually means on a clinical level. Put simply, mixed hyperlipidemia is a metabolic condition where a patient’s blood carries abnormally high levels of both cholesterol and triglycerides at the same time. This sets it apart from pure hypercholesterolemia, where only cholesterol rises, and from pure hypertriglyceridemia, where only triglycerides cause the problem.
This condition develops primarily because elevated low-density lipoproteins (LDL) and very-low-density lipoproteins (VLDL) flood the bloodstream. When the body fails to clear these lipoproteins efficiently, fats accumulate in the blood, driving up the risk of arterial plaques, heart attacks, strokes, and peripheral artery disease. This is exactly why accurate diagnosis and coding through the hyperlipidemia ICD 10 system matters so much. It goes beyond paperwork. It forms the backbone of appropriate treatment planning.
One important clinical reality: mixed hyperlipidemia often stays completely silent. Many patients show zero noticeable symptoms until the disease progresses to a point where cardiovascular risk becomes serious. A routine fasting lipid panel blood test remains the primary tool for catching it early.
Common Causes and Risk Factors
Mixed hyperlipidemia develops through two main pathways: genetic and acquired. Understanding these causes helps clinicians document the right diagnosis, which in turn supports proper code assignment.
Genetic causes drive a large number of cases. Familial combined hyperlipidemia, often shortened to FCH, ranks among the most common inherited lipid disorders. It affects roughly 1 to 2 percent of the general population and produces a variable pattern of elevated plasma cholesterol and triglycerides. Mutations in the receptor-binding domain of apolipoprotein B-100, a key component of LDL and VLDL, reduce the body’s ability to clear these lipoproteins, pushing levels upward over time.
Acquired causes include conditions like uncontrolled Type 2 diabetes, hypothyroidism, kidney disease, and certain medications such as corticosteroids and beta-blockers. Poor dietary habits and a sedentary lifestyle also contribute in major ways. In many real-world cases, patients bring both a genetic predisposition and lifestyle factors to the table, making thorough clinical assessment and detailed documentation critical for correct mixed hyperlipidemia ICD 10 code assignment.
Breaking Down E78.2: What the Code Covers
The ICD-10-CM E78.2 code captures several specific clinical scenarios. The ICD-10 inclusion terms under this code cover:
- Combined hyperlipidemia, not otherwise specified (NOS)
- Elevated cholesterol with elevated triglycerides, not elsewhere classified (NEC)
- Fredrickson Type IIb hyperlipoproteinemia
- Hyperlipidemia, Group C
- Hyperbetalipoproteinemia with pre-beta-lipoproteinemia
- Xanthoma tuberosum
All of these terms point to the same underlying clinical reality: both cholesterol and triglycerides rise together. So when a provider documents any of these terms in the patient record, E78.2 becomes the correct code to assign.
Important Exclusions You Need to Know
Using E78.2 correctly also means knowing what it does NOT cover. A Type 1 Excludes note attaches to this code, meaning the excluded conditions must never pair with E78.2 on the same claim. Specifically:
- Cerebrotendinous cholesterosis (van Bogaert-Scherer-Epstein disease) belongs to E75.5, not E78.2.
- Familial combined hyperlipidemia belongs to E78.49, not E78.2.
- Sphingolipidosis codes (E75.0 through E75.3) must also stay separate from E78.2.
Additionally, when a patient carries both mixed hyperlipidemia and pure hypercholesterolemia, you should only assign E78.2. Do not add E78.00 separately. The hypercholesterolemia ICD 10 component already lives inside E78.2, so coding both creates a duplicate entry and can trigger an audit.
How E78.2 Differs from Other Hyperlipidemia ICD 10 Codes
Distinguishing between the different lipid disorder codes trips up even experienced coders. Here is a clean breakdown to help you pick the right one every single time.
E78.00 — Pure Hypercholesterolemia, Unspecified Use this when lab results show elevated LDL or total cholesterol only, with triglyceride levels sitting within a normal range. This code serves as the standard hypercholesterolemia ICD 10 option.
E78.1 — Pure Hypertriglyceridemia This code fits when only triglycerides ICD 10 climbs above normal and cholesterol stays within range. Think of this as the isolated high-triglyceride code.
E78.2 — Mixed Hyperlipidemia Reach for this code whenever both LDL cholesterol and triglycerides rise together. This is the combined hyperlipidemia diagnosis code that clearly signals a dual-lipid problem to payers and reviewers.
E78.49 — Other Hyperlipidemia Choose this when the provider documents a specific lipid abnormality, but ICD-10 lacks a dedicated code for it, such as elevated non-HDL cholesterol as the primary concern.
E78.5 — Hyperlipidemia, Unspecified The E78.5 diagnosis code belongs in situations where the provider documents hyperlipidemia but does not specify the exact type. This code works as a fallback option only. Never swap it in for E78.2 when documentation clearly supports both elevated cholesterol and triglycerides. Making that substitution counts as a coding error and can lead to claim denials.
Documentation Requirements for E78.2
Strong documentation drives accurate coding. When it comes to the ICD-10 code for mixed hyperlipidemia, the medical record needs to include all of the following elements to fully support the diagnosis:
Laboratory Results: A recent fasting lipid panel showing both LDL cholesterol and triglyceride levels above normal ranges. Documentation like “LDL-C 185 mg/dL, triglycerides 320 mg/dL” gives exactly the level of specificity that supports E78.2 and holds up under review.
Clinical Context: Physician notes from the physical examination, along with patient history, symptoms, and identified risk factors, must accompany the lab findings.
Diagnostic Confirmation: The provider must explicitly confirm that both lipid components have risen above normal. If the provider mentions only high triglycerides, E78.1 fits better than E78.2.
Treatment Plan: The record should clearly show any prescribed medications, such as statins or fibrates, along with lifestyle modification recommendations. This documentation reinforces the clinical importance of the diagnosis and strengthens the claim.
Missing lab documentation stands out as the single most common reason that E78.2 claims get flagged during audits. Always attach the lab results to the record before submitting.
How to Use E78.2 for Billing and Reimbursement
From a billing standpoint, E78.2 operates as a billable, specific ICD-10-CM code. That means you can submit it directly on insurance claims without needing an additional manifestation code. Claims carrying E78.2 stay valid for all HIPAA-covered transactions during fiscal year 2026.
When mixed hyperlipidemia appears alongside other conditions like Type 2 diabetes (commonly coded as E11.69) or hypertension, assign additional codes to capture all comorbidities. Code sequencing matters here. Generally, the condition driving the visit goes first. So if the patient comes in specifically to manage lipid levels, E78.2 leads the claim, followed by any related conditions.
Many practices also pair E78.2 with CPT Code 80061 for the lipid panel test that confirms the diagnosis. This test measures total cholesterol, HDL, LDL, and triglycerides together in a single blood draw, making it the standard diagnostic tool for mixed hyperlipidemia. For follow-up office visits managing this condition, CPT Code 99214 commonly covers moderate-complexity evaluations.
Treatment Overview for Mixed Hyperlipidemia
While this guide focuses primarily on coding, treatment documentation also directly supports E78.2 claims. Effective management of mixed hyperlipidemia combines lifestyle changes with targeted medications.
Lifestyle changes take the front line. A heart-healthy diet that cuts saturated fats, trans fats, and refined sugars brings down both cholesterol and triglyceride levels meaningfully. Regular aerobic exercise further improves lipid profiles over time. Clinicians who document specific dietary and exercise guidance provide stronger support for the diagnosis and treatment plan together.
Medications enter the picture when lifestyle changes alone fall short. Statins lead the way in lowering LDL cholesterol across most patient populations. Fibrates, such as fenofibrate, target elevated triglycerides specifically and work well alongside statins in many cases. Prescription-dose omega-3 fatty acid supplements also lower triglycerides effectively for many patients. Documenting the specific medications prescribed, along with the clinical rationale, further strengthens the E78.2 claim and reduces denial risk.
Frequently Asked Questions (FAQs)
Q1: What is the ICD-10 code for mixed hyperlipidemia?
The ICD-10 code for mixed hyperlipidemia is E78.2. Physicians and coders use this billable, specific diagnosis code when a patient presents with both elevated cholesterol and elevated triglycerides. The 2026 edition of this code took effect on October 1, 2025.
Q2: What is the difference between E78.2 and E78.5?
E78.2 applies specifically when documentation confirms both elevated cholesterol and elevated triglycerides. The E78.5 diagnosis code covers unspecified hyperlipidemia, meaning the provider did not document the type. Always choose E78.2 over E78.5 whenever lab results confirm a dual-lipid problem.
Q3: Can I code E78.00 and E78.2 together?
No. When a patient has both mixed hyperlipidemia and hypercholesterolemia, only assign E78.2. The hypercholesterolemia ICD 10 component already lives within the E78.2 code definition. Coding both codes together creates a duplication error that can trigger claim reviews.
Q4: What is the ICD-10 code for high triglycerides only?
When only triglycerides climb above normal while cholesterol remains within range, the correct code is E78.1, which covers pure hypertriglyceridemia. This serves as the correct triglycerides ICD 10 code for isolated high-triglyceride cases.
Q5: Is familial combined hyperlipidemia coded as E78.2?
No. Although familial combined hyperlipidemia involves a mixed lipid pattern, its correct ICD-10 code is E78.49 under “other hyperlipidemia.” A Type 1 Excludes note on E78.2 explicitly directs coders away from using E78.2 for familial combined hyperlipidemia.
Q6: What documentation supports an E78.2 claim?
You need lab results showing both elevated LDL cholesterol and triglycerides, physician notes confirming the diagnosis, a clinical history with relevant risk factors, and a documented treatment plan. Missing lab documentation triggers the most common audit flags for this code.
Q7: Can E78.2 pair with a diabetes diagnosis code?
Yes. Mixed hyperlipidemia frequently coexists with Type 2 diabetes. In those cases, assign E78.2 alongside the appropriate diabetes code such as E11.69. Always follow ICD-10 sequencing guidelines to determine which diagnosis leads the claim based on the primary reason for the visit.
This article serves informational purposes related to medical coding and clinical documentation. Always consult current ICD-10-CM official guidelines and your organization’s compliance policies before making specific coding decisions.