E78.00 ICD-10: The Code Every Coder and Biller Needs to Know
If you work in medical coding, billing, or clinical documentation, you deal with cholesterol-related diagnoses almost every single day. Cardiovascular disease remains the number one killer in the United States, and high cholesterol sits at the center of that story. So let’s get straight to the point: E78.00 ICD-10 stands for “Pure hypercholesterolemia, unspecified,” and it ranks as one of the most frequently billed diagnosis codes in primary care, cardiology, and endocrinology practices nationwide.
The 2026 edition of this code took effect on October 1, 2025, and it stays valid for all HIPAA-covered transactions through September 30, 2026. Physicians, coders, and billers across the country rely on E78.0 ICD 10 and its subcodes daily to document isolated elevated cholesterol and push clean claims through payer systems.
Getting this code right matters beyond just passing a claim. It directly shapes reimbursement, DRG assignment, chronic care management eligibility, risk adjustment scores, and the clinical accuracy of your patient records. Using a vague or incorrect code when the documentation clearly supports a specific one is a coding error that invites denials and audit flags.
What Does E78.00 Actually Mean? The Clinical Picture First
Before diving into coding mechanics, let’s make sure the clinical foundation is solid. Pure hypercholesterolemia describes a condition where a patient carries abnormally high levels of cholesterol in the blood, specifically elevated low-density lipoprotein (LDL), without a corresponding elevation of triglycerides or other lipid abnormalities. This is what makes it “pure.” Only cholesterol rises. Triglycerides and other lipid components stay within normal ranges.
The word “unspecified” in the full code title tells you something critical: the provider documented elevated LDL cholesterol without clarifying whether a genetic mutation, lifestyle factor, or secondary medical condition drives the problem. That unspecified status makes E78.00 the right call when the documentation shows high cholesterol but does not identify the root cause or type.
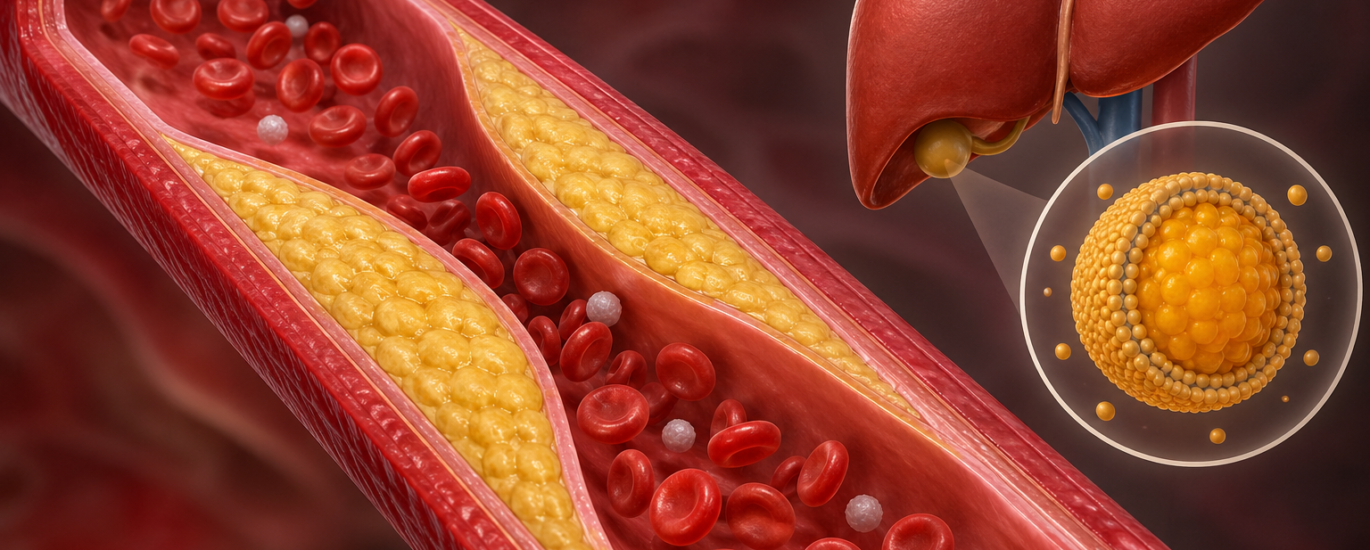
Cholesterol itself is not the villain. Your body needs it to build cell membranes, produce hormones like estrogen and testosterone, and synthesize vitamin D. The problem starts when LDL levels climb too high and begin depositing fatty plaques along artery walls, a process called atherosclerosis. Over time, these plaques narrow the arteries, restrict blood flow, and dramatically raise the risk of heart attack, stroke, and peripheral artery disease.
Why High Cholesterol Often Goes Undetected
One of the most important clinical facts about hypercholesterolemia is that it produces no noticeable symptoms on its own. Patients feel completely fine while their LDL silently builds up plaques over years or even decades. A routine fasting lipid panel, which measures total cholesterol, LDL, HDL, and triglycerides together through a simple blood draw, catches the condition before it progresses to cardiovascular damage. This is exactly why primary care providers order lipid panels so routinely, and why the ICD code for high cholesterol shows up on claims at such high volumes.
The Full E78.0 Code Family: Breaking Down Every Subcode
The E78.0 ICD 10 category covers pure hypercholesterolemia and breaks into several specific subcodes depending on what the provider documents. Understanding each one prevents the costly mistake of assigning an unspecified code when a more precise option clearly applies.
E78.00 — Pure Hypercholesterolemia, Unspecified
Use this code when the provider documents high cholesterol, pure hypercholesterolemia, elevated LDL, or hypercholesterolemia ICD 10 without identifying whether a genetic cause or specific secondary trigger drives the elevation. The diagnosis code E7800 serves as the go-to option for the vast majority of straightforward high-cholesterol cases in general practice.
Inclusion terms that map directly to this code include:
- Pure hypercholesterolemia NOS (not otherwise specified)
- Fredrickson’s hyperlipoproteinemia, Type IIa
- Hyperbetalipoproteinemia
- Low-density-lipoprotein-type (LDL) hyperlipoproteinemia
All of these terms point to the same clinical reality: elevated LDL without accompanying triglyceride elevation and without a specified genetic mutation. So when a provider writes “LDL cholesterol 210 mg/dL, starting rosuvastatin,” E78.00 fits perfectly.
E78.01 — Familial Hypercholesterolemia
This subcode steps up in specificity and covers cases where a genetic mutation drives the cholesterol elevation. Familial hypercholesterolemia (FH) is an inherited condition where a defect in the LDL receptor gene prevents the liver from clearing LDL from the bloodstream efficiently. This causes dramatically elevated LDL levels, often above 190 mg/dL, from birth onward, and it carries a very high lifetime risk of premature cardiovascular events.
When the provider documents familial hypercholesterolemia specifically, or when genetic testing confirms the diagnosis, move past E78.00 and assign one of the E78.01 subcodes:
- E78.010 — Homozygous familial hypercholesterolemia (HoFH): The patient inherited the defective gene from both parents. LDL levels often exceed 400 mg/dL, and cardiovascular events can occur in childhood. This is a severe, rare form.
- E78.011 — Heterozygous familial hypercholesterolemia (HeFH): The patient inherited the defective gene from one parent. This is far more common, affecting roughly 1 in 250 people in the U.S., and it significantly raises cardiovascular risk compared to garden-variety high cholesterol.
- E78.019 — Familial hypercholesterolemia, unspecified: Use this when the provider confirms the familial type but does not specify homozygous or heterozygous status.
The distinction between E78.00 and E78.01 carries real consequences. Familial hypercholesterolemia codes support medical necessity for more aggressive lipid-lowering treatment, including PCSK9 inhibitors like evolocumab and alirocumab, and in some cases lipoprotein apheresis. Assigning E78.00 when the provider has clearly documented familial FH leaves clinical information on the table and can lead to prior authorization denials for high-cost specialty drugs.
How E78.00 Differs from Other High Cholesterol and Hyperlipidemia Codes
One of the most consistent mistakes in lipid disorder coding involves mixing up codes across the E78 family. Here is a clean side-by-side comparison that eliminates the confusion.
E78.00 vs. E78.5 — The Most Common Mistake
The ICD code 10 for hypercholesterolemia that coders most frequently assign incorrectly is E78.5, “Hyperlipidemia, unspecified.” Many coders default to E78.5 out of habit, especially when provider documentation feels thin. However, when the record clearly shows that only cholesterol runs high and triglycerides sit within normal range, E78.00 fits the picture precisely. Using E78.5 instead of E78.00 in that scenario counts as a coding error.
E78.5 belongs in the record only when the provider documents hyperlipidemia without specifying the type, and when the lipid panel does not provide enough clarity to support a more specific code. Overuse of E78.5 triggers payer scrutiny, reduces clinical data accuracy, and can affect risk adjustment scores for value-based care contracts.
E78.00 vs. E78.2 — Cholesterol Alone vs. Both Lipids
E78.2 covers mixed hyperlipidemia, the condition where both LDL cholesterol and triglycerides rise above normal ranges simultaneously. Never use E78.00 and E78.2 together. When both lipids elevate, E78.2 captures the full picture. When only LDL rises, E78.00 applies. Always check the lipid panel values carefully before selecting between these two.
E78.00 vs. E78.1 — High Cholesterol vs. High Triglycerides
E78.1 covers pure hypertriglyceridemia, where only triglycerides climb above normal while cholesterol stays in range. These two codes sit at opposite ends of the lipid spectrum and should never confuse an experienced coder. E78.00 targets LDL. E78.1 targets triglycerides. The lipid panel tells you which one applies.
Critical Coding Rules for E78.00
Applying E78.00 ICD 10 correctly demands following several specific guidelines that protect claims from denials and audit risk. Here are the rules that matter most in 2026.
Never Code from Lab Values Alone
ICD-10-CM guidelines prohibit coders from assigning E78.00 based solely on an elevated LDL value in a lab report without a provider-confirmed diagnosis. The provider must explicitly document high cholesterol, hypercholesterolemia, or pure hypercholesterolemia in the assessment or problem list. An LDL of 195 mg/dL sitting in the lab section of the record without a corresponding provider statement does not support E78.00 coding.
Do Not Use a Decimal Point on Electronic Claims
This is a practical billing tip that catches a lot of practices off guard. When submitting claims electronically, enter the code as E7800 without a decimal point. Some clearinghouses strip the decimal automatically, but many systems reject claims containing a decimal in the diagnosis code field. The decimal appears in the ICD-10-CM tabular for readability, but it does not belong in electronic claim data. Always submit as E7800.
Choose Specificity Over Convenience
When provider documentation supports E78.01 for familial hypercholesterolemia but the coder settles for E78.00 because it is faster to assign, that choice creates clinical and compliance risk. Push providers to document specifically whether the condition is familial or acquired, and then assign the code that matches the documentation. Specific codes pass through payers more cleanly and support stronger medical necessity arguments.
Pair E78.00 with Comorbidity Codes Correctly
High cholesterol frequently travels alongside other chronic conditions. Coders should assign companion codes to paint the full clinical picture:
- Z79.899 — Other long-term (current) drug therapy: Add this when the patient takes statins or other cholesterol-lowering medications on a long-term basis. This code documents ongoing treatment and supports medical necessity for follow-up visits.
- E11.65 — Type 2 diabetes with hyperglycemia: When high cholesterol coexists with diabetes, assign both codes. Hypercholesterolemia accelerates cardiovascular risk in diabetic patients, and payers expect to see this documented together.
- I10 — Essential (primary) hypertension: Hypertension and high cholesterol frequently coexist, and documenting both codes together tells a more complete cardiovascular risk story.
- Z82.49 — Family history of ischemic heart disease and other diseases of the circulatory system: When family history drives the clinical concern, this Z code adds valuable context to the E78.00 claim.
Documentation Requirements That Make E78.00 Audit-Proof
Strong documentation protects your claims and strengthens the clinical record at the same time. For E78.00, the medical record should include all of the following elements before submission:
An explicit provider diagnosis statement. The assessment or problem list must use terms like “high cholesterol,” “hypercholesterolemia,” or “pure hypercholesterolemia.” The provider’s diagnostic statement carries more weight than lab values alone.
A recent lipid panel with results. Lab values showing LDL above 130 mg/dL, alongside normal triglyceride levels, support the pure hypercholesterolemia diagnosis and confirm that E78.00 rather than E78.2 applies.
Ruling out or confirming familial causes. If the provider reviewed family history or ordered genetic testing, document those findings. If familial causes are not present or not suspected, a brief note confirming that secondary causes were considered strengthens the clinical record significantly.
A treatment plan. Document whether the patient starts a statin, adjusts an existing medication dose, or pursues lifestyle modifications. Recording the treatment plan confirms the clinical relevance of the diagnosis and supports the E/M visit level.
Medication reconciliation. Note any existing cholesterol-lowering drugs the patient currently takes, including the drug name, dose, and duration. This supports chronic condition management coding and demonstrates ongoing clinical engagement with the diagnosis.
Treatment Context That Supports Your E78.00 Claims
Coders who understand how providers treat hypercholesterolemia ICD 10 cases can better verify that the documentation matches the code and the visit level billed. Providers managing E78.00 patients typically pursue a layered approach:
Lifestyle modification always comes first. Dietary changes that reduce saturated fats and trans fats, increase soluble fiber, and emphasize plant-based foods bring LDL down meaningfully. Regular aerobic exercise raises HDL while lowering LDL. Smoking cessation removes a major cardiovascular risk amplifier. Documenting these recommendations in the record, even briefly, shows active clinical management.
Statins lead the pharmacological fight. Drugs like atorvastatin, rosuvastatin, and simvastatin block HMG-CoA reductase, the enzyme the liver uses to produce cholesterol. This forces the liver to pull more LDL from the bloodstream, lowering circulating levels. Statins reduce the risk of heart attack and stroke across most patient populations, making them the cornerstone of pharmacological treatment for E78.00 patients.
Add-on therapies handle statin-resistant cases. Ezetimibe blocks cholesterol absorption in the small intestine and pairs well with statins. For high-risk patients whose LDL does not respond adequately to statin therapy, PCSK9 inhibitors offer powerful additional LDL reduction, though prior authorization requirements make accurate coding critical for these patients.
Monitoring drives ongoing visit documentation. Providers order repeat lipid panels four to twelve weeks after initiating or adjusting therapy to verify response. These follow-up visits generate ongoing E78.00 claims and require the same documentation standards as the initial visit.
Frequently Asked Questions (FAQs)
Q1: What is the E78.00 ICD-10 code?
E78.00 is the ICD-10-CM code for pure hypercholesterolemia, unspecified. Providers and coders use this billable code when a patient carries elevated LDL cholesterol without elevated triglycerides and without a confirmed genetic cause. The 2026 edition took effect on October 1, 2025, and stays valid through September 30, 2026.
Q2: What is the difference between E78.00 and E78.01?
E78.00 covers pure hypercholesterolemia when the provider does not identify a genetic cause. E78.01 covers familial hypercholesterolemia, a genetic form where a defective LDL receptor gene causes severely elevated cholesterol. When genetic testing or documented family history confirms the familial diagnosis, E78.01 replaces E78.00. Using E78.00 instead of E78.01 when familial FH is clearly documented counts as under-coding.
Q3: What is the ICD code for high cholesterol that doctors use most often?
The most commonly used ICD code for high cholesterol in clinical practice is E78.00 for pure hypercholesterolemia and E78.5 for unspecified hyperlipidemia. E78.00 applies when only cholesterol rises and no specific type is identified. E78.5 applies when the provider documents hyperlipidemia without specifying whether cholesterol, triglycerides, or both drive the abnormality.
Q4: Should I use E78.00 or E78.5 for a patient with high LDL only?
Use E78.00. When the lipid panel shows elevated LDL with normal triglycerides, and the provider documents high cholesterol or hypercholesterolemia, E78.00 fits precisely. Reserve E78.5 for situations where the provider documents hyperlipidemia without specifying the type, or when the record does not provide enough detail to support a more specific code.
Q5: What does the diagnosis code E7800 mean on a claim form?
Diagnosis code E7800 on an electronic claim form represents pure hypercholesterolemia, unspecified, the same condition as E78.00 in the ICD-10 tabular list. Electronic claim submission systems require the code without a decimal point, so E7800 and E78.00 refer to exactly the same diagnosis. Always drop the decimal when submitting electronically to avoid claim rejections.
Q6: Can E78.00 and E78.5 appear on the same claim?
No. These two codes cover overlapping clinical territory, and assigning both on the same claim creates a duplication error. When documentation supports E78.00 specifically, use that code alone. Only reach for E78.5 when specificity is genuinely unavailable from the provider’s documentation.
Q7: Does E78.00 require a companion code for statin therapy?
ICD-10-CM does not mandate a companion code for statin therapy, but adding Z79.899 for long-term drug therapy significantly strengthens the claim. It documents ongoing treatment, supports medical necessity for follow-up management visits, and demonstrates active clinical engagement with the chronic condition. Many experienced coders add it routinely when the patient takes statins.
Q8: What CPT codes commonly pair with E78.00?
CPT Code 80061 for a lipid panel pairs with E78.00 when the provider orders the diagnostic test. For office visit management of high cholesterol, CPT codes 99213 and 99214 cover low-to-moderate and moderate complexity encounters respectively. For high-risk patients requiring longer discussions of cardiovascular risk and treatment adjustment, 99214 or 99215 typically fits the documentation.
This article provides informational guidance on ICD-10-CM coding for educational purposes. Always apply current official ICD-10-CM guidelines and your organization’s compliance policies when making specific coding decisions.