

If you’re a medical coder, biller, or clinician who deals with spine conditions daily, you already know how messy spinal stenosis coding can get. One wrong digit and your claim bounces right back. So let’s cut through the noise and give you a complete, no-fluff breakdown of the ICD-10 code for cervical spinal stenosis — updated for 2026, plain-English style.
In this guide, we cover the correct codes, when to use each one, how to avoid the most common billing mistakes, what changed in the 2026 update, and how cervical stenosis coding connects to related conditions like lumbar stenosis ICD-10, neural foraminal stenosis ICD-10, and lumbosacral stenosis ICD-10. Let’s get into it.
What Is Cervical Spinal Stenosis — And Why the Right Code Matters
Cervical spinal stenosis is a condition where the spinal canal in the neck region narrows, squeezing the spinal cord and nerve roots. This narrowing creates a whole cascade of symptoms that range from annoying to outright debilitating. The condition mostly affects adults over 50, though congenital cases do pop up in younger patients.
From a coding standpoint, getting this diagnosis right is not just about accuracy — it directly affects your reimbursement rate, your audit risk, and whether or not your claim gets paid the first time. In fact, cervical spine claims are among the most frequently audited categories in musculoskeletal billing. So yeah, this stuff matters a lot.
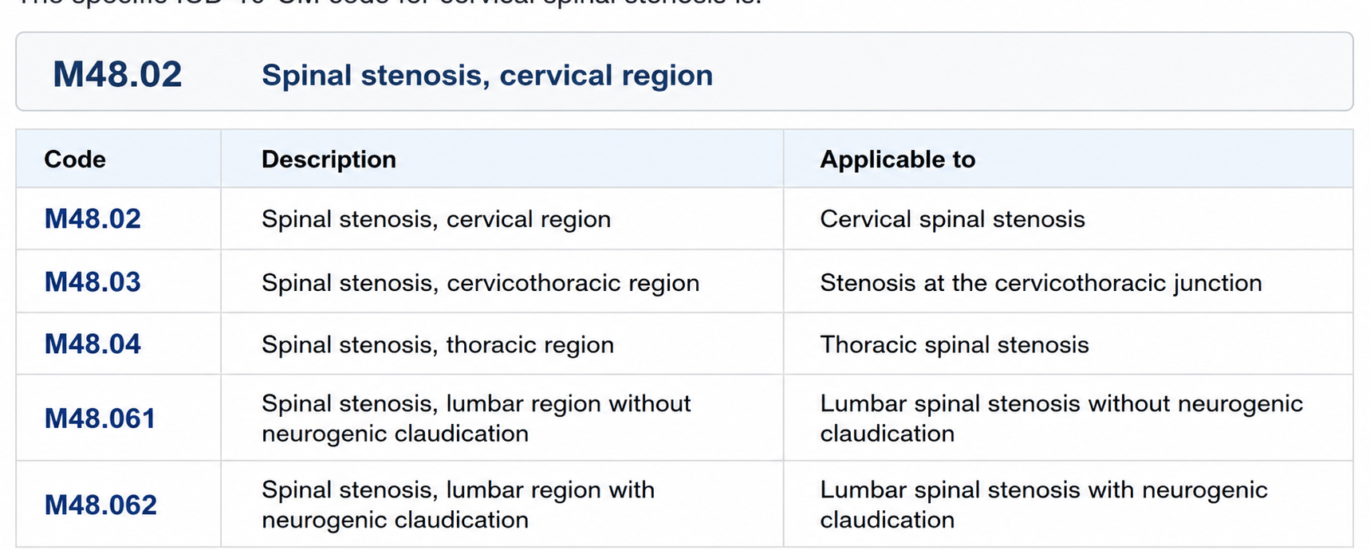
The ICD-10-CM code M48.02 specifically captures spinal stenosis in the cervical region. It falls under the broader category M48 — “Other spondylopathies” — which covers conditions of the vertebrae that aren’t inflammatory in nature. The cervical region, for coding purposes, refers to the neck area of the spine (vertebrae C1 through C7).
M48.02 covers both central canal stenosis and foraminal stenosis in the cervical region. ICD-10-CM does not create a separate distinction between the two at the cervical level — so one code handles both.
Symptoms of Cervical Spinal Stenosis
Understanding the clinical picture helps coders choose the right code with confidence. Plus, documentation of these symptoms directly supports medical necessity. Here’s what patients with cervical stenosis typically present with:
- Neck pain that worsens with movement or extension
- Radiating pain, numbness, or tingling down one or both arms (radiculopathy)
- Weakness in the hands, arms, or fingers — often described as dropping things
- Balance problems and coordination difficulty (a big red flag for myelopathy)
- Electric shock sensations running down the back when bending the neck forward (Lhermitte’s sign)
- Bladder or bowel dysfunction in severe cases
- Muscle spasms in the neck and upper back
Here’s the key thing — if the physician documents myelopathy (spinal cord compression symptoms like balance issues and weakness), that opens up a different coding pathway compared to simple stenosis without neurological involvement. More on that in the related codes section below.
What Causes Cervical Spinal Stenosis?
Coders should understand the root causes because sometimes the underlying condition drives the code choice, especially when a more specific code exists for that etiology.
- Degenerative disc disease — the most common cause, especially in older adults
- Bone spurs (osteophytes) that grow into the spinal canal
- Ligamentum flavum thickening and hypertrophy
- Herniated cervical discs pressing on the cord or nerve roots
- Spondylosis — general age-related degeneration of the cervical vertebrae
- Congenital narrow spinal canal (less common, but possible)
- Trauma or injury to the cervical spine causing post-traumatic stenosis
- Rheumatoid arthritis affecting the cervical joints
When degenerative changes are documented as the primary driver, coders sometimes need to consider codes from the M47 range (spondylosis) rather than jumping straight to M48.02. The physician’s documentation is always your guiding star here.
The Primary ICD-10 Code for Cervical Spinal Stenosis
| ICD-10 Code | Description | Status | When To Use |
|---|---|---|---|
| M48.02 | Spinal stenosis, cervical region | ✔ Billable 2026 | Primary diagnosis for cervical canal or foraminal narrowing without specifying myelopathy |
| M47.12 | Other spondylosis with myelopathy, cervical region | ✔ Billable 2026 | When spondylosis-driven stenosis presents with documented myelopathy |
| M54.12 | Radiculopathy, cervical region | ✔ Billable 2026 | Add as secondary code when radiculopathy is documented alongside M48.02 |
| M99.41 | Connective tissue stenosis of neural canal of cervical region | ✔ Billable 2026 | Use when stenosis is specifically due to connective tissue — typically a chiropractic coding scenario |
| M99.71 | Connective tissue and disc stenosis of intervertebral foramina, cervical region | ✔ Billable 2026 | Foraminal narrowing from disc and connective tissue combined in cervical region |
Related Spinal Stenosis ICD-10 Codes You Need to Know
Cervical stenosis doesn’t exist in a vacuum. Patients often have multi-level disease, and billers frequently need to code conditions at other spinal levels too. Here’s your complete reference for the related spinal stenosis ICD-10 landscape in 2026.
Spinal Stenosis ICD-10 Codes by Region
| ICD-10 Code | Description | Effective |
|---|---|---|
| M48.01 | Spinal stenosis, occipito-atlanto-axial region | 2026 |
| M48.02 | Spinal stenosis, cervical region | 2026 |
| M48.03 | Spinal stenosis, cervicothoracic region | 2026 |
| M48.04 | Spinal stenosis, thoracic region | 2026 |
| M48.06 | Spinal stenosis, lumbar region (lumbar stenosis ICD-10) | 2026 |
| M48.061 | Lumbar stenosis without neurogenic claudication | 2026 |
| M48.062 | Lumbar stenosis with neurogenic claudication | 2026 |
| M48.07 | Spinal stenosis, lumbosacral region (lumbosacral stenosis ICD-10) | 2026 |
| M99.63 | Neural foraminal stenosis — osseous, lumbar region | 2026 |
| M99.71 | Neural foraminal stenosis — disc & connective tissue, cervical region | 2026 |
Neural Foraminal Stenosis ICD-10 — Breaking It Down
Neural foraminal stenosis ICD-10 coding is its own mini-world. The neural foramen is the small opening through which the nerve root exits the spinal canal. When it narrows, it specifically compresses individual nerve roots — producing classic radiculopathy symptoms like shooting arm or leg pain.
For the cervical region, foraminal stenosis falls under M48.02 since ICD-10-CM does not separate central canal stenosis from foraminal stenosis at that level. For the lumbar region, the more specific code M99.63 applies for osseous foraminal stenosis, while M99.71 covers the cervical foraminal variant when connective tissue and disc involvement is the driver.
Lumbosacral Stenosis ICD-10 — Know the Difference
Lumbosacral stenosis ICD-10 code M48.07 is specifically for the junction between the lumbar spine and the sacrum — the L5-S1 area. This is distinct from plain lumbar stenosis (M48.06). Getting this distinction wrong is a super common audit trigger, so always check the physician’s documentation to see exactly where the stenosis sits anatomically.
Billing Tips for Cervical Spinal Stenosis — Get Paid Right
Let’s get practical. Here are the real-world billing tips that experienced coders use to keep claims clean and reimbursements flowing.
- Always tie the code to imaging. M48.02 needs to be backed by an MRI or CT scan report documenting the stenosis. Make sure the radiology report is in the chart before you submit.
- Code the myelopathy when it’s there. If the physician documents myelopathy — balance problems, hand clumsiness, or cord signal changes on MRI — use M47.12, not just M48.02. Myelopathy bumps your claim into a higher-acuity DRG group.
- Add radiculopathy as a secondary code. When radiculopathy is separately documented, code M54.12 alongside M48.02. These two codes stack legally because they represent distinct clinical findings.
- Never use M48.0 (the parent code) for billing. M48.0 is the non-billable parent. M48.02 is the specific, billable child code for the cervical region. Using the parent code gets you denied immediately.
- Match your CPT codes to the diagnosis. For surgical cases like ACDF (anterior cervical discectomy and fusion), your ICD-10 diagnosis codes must clearly establish medical necessity. M48.02 paired with documented neurological involvement is your strongest foundation.
- Watch out for laterality gaps. Unlike some musculoskeletal codes, ICD-10 does not require laterality for spinal stenosis codes. Don’t stress about left vs. right — the region is enough.
Pro Billing Tip: For Medicare patients, cervical stenosis procedures often require a signed ABN (Advance Beneficiary Notice) when medical necessity is borderline. Always confirm payer-specific LCD (Local Coverage Determination) requirements before submitting spine-related claims.
Common Coding Mistakes — And How to Avoid Them
These mistakes show up constantly in audits and claim denials. Fix them now.
- Using the unspecified code M48.9. This is a lazy fallback. Auditors flag it immediately. Always dig into the documentation and find the region-specific code.
- Coding herniated disc as stenosis. If the stenosis is directly caused by a herniated disc, you may need a disc code (M50 series for cervical) alongside or instead of M48.02. Don’t assume they’re always interchangeable.
- Skipping the secondary radiculopathy code. Many coders forget M54.12 when it’s clearly documented. That’s lost specificity and sometimes lost reimbursement.
- Confusing lumbosacral (M48.07) with lumbar (M48.06). These are completely different codes for different regions. Check the imaging report — L5-S1 involvement means lumbosacral, not just lumbar.
- Coding myelopathy under M48.02 instead of M47.12. M48.02 doesn’t capture spondylogenic myelopathy. If the cord is compressed from degenerative spondylosis plus stenosis, M47.12 is your primary.
- Failing to document medical necessity for surgery. ICD-10 codes alone won’t save you if the clinical notes don’t support why the procedure was necessary. The diagnosis code and the chart need to tell the same story.
2026 ICD-10-CM Updates — What’s New for Spinal Stenosis Coding
Effective October 1, 2025 — For 2026 Billing Year
The 2026 edition of ICD-10-CM became effective on October 1, 2025. Here’s what coders need to know specifically around spinal stenosis coding this cycle.
Key 2026 Updates at a Glance
- M48.02 remains fully valid and billable — no changes to the code itself this cycle
- The MS-DRG v43.0 grouper now applies to M48.02, grouping it within DRGs 551 (Medical back problems with MCC) and 552 (without MCC)
- M48.061 and M48.062 (lumbar stenosis with and without neurogenic claudication) remain the gold standard for lumbar stenosis ICD-10 specificity — no rollback to M48.06 as a standalone billable option
- Payer scrutiny on spinal surgery medical necessity has intensified in 2026 — solid ICD-10 documentation is more critical than ever
- AI-assisted coding tools are now widely adopted by major health systems, but human review remains essential for cervical spine diagnoses due to the complexity of overlapping conditions
2026 Practice Note: CMS has placed spine procedures under increased post-payment review in 2026. Make sure every cervical stenosis claim includes imaging documentation, symptom duration, conservative treatment tried, and clear indication for the level of care provided.
DRG Grouping Impact for Cervical Stenosis
Under MS-DRG v43.0, M47.12 (cervical spondylosis with myelopathy) groups into DRGs 551/552 — the “Medical back problems” category. This matters for inpatient billing because the presence of an MCC (Major Complicating Condition) shifts the case to the higher-paying DRG 551. So when your patient has myelopathy plus another significant comorbidity, make sure both are coded correctly. That difference can represent hundreds of dollars per case.
Frequently Asked Questions (FAQ)
What is the ICD-10 code for cervical spinal stenosis?
The correct ICD-10 code for cervical spinal stenosis is M48.02 — “Spinal stenosis, cervical region.” It is a billable, specific code under the 2026 ICD-10-CM edition, effective October 1, 2025. It covers both central canal and foraminal stenosis in the cervical (neck) region.
What is the difference between M48.02 and M47.12?
M48.02 is used for spinal stenosis of the cervical region as the primary pathology. M47.12 applies when spondylosis (degenerative joint disease) is the driver and myelopathy (spinal cord involvement) is present. If your patient has cord compression symptoms like gait problems or hand weakness, M47.12 is typically more appropriate as the principal diagnosis.
What is the lumbar stenosis ICD-10 code for 2026?
The lumbar stenosis ICD-10 codes for 2026 are M48.061 (lumbar stenosis without neurogenic claudication) and M48.062 (lumbar stenosis with neurogenic claudication). The parent code M48.06 exists but is non-billable — you must use the specific seventh-character extension codes.
What is the neural foraminal stenosis ICD-10 code?
For neural foraminal stenosis, the code depends on the spinal region. In the cervical region, M48.02 covers foraminal stenosis. In the lumbar region, M99.63 (osseous and subluxation stenosis of intervertebral foramina, lumbar region) or M48.061/M48.062 applies depending on the clinical presentation.
What is the lumbosacral stenosis ICD-10 code?
The lumbosacral stenosis ICD-10 code is M48.07 — “Spinal stenosis, lumbosacral region.” It became effective October 1, 2025 under the 2026 ICD-10-CM edition and specifically captures stenosis at the L5-S1 junction region.
Can I bill M48.02 and M54.12 together?
Yes. These two codes are commonly billed together when the patient has both cervical stenosis and documented cervical radiculopathy. M48.02 is the principal diagnosis (the stenosis), and M54.12 is the secondary code capturing the radiculopathy. There is no Excludes 1 note preventing their combined use.
Is cervical spinal stenosis coding different for surgical vs. non-surgical claims?
The diagnosis code M48.02 itself stays the same regardless of whether the claim is for surgery, physical therapy, or imaging. What changes is what you must document to establish medical necessity for each level of care. For surgery, you need clear evidence of failed conservative treatment, neurological deficit, or significant functional impairment tied to the stenosis diagnosis.
Wrapping It Up — Code It Right, Get Paid Right
Understanding the ICD-10 code for cervical spinal stenosis goes way beyond memorizing M48.02. It means knowing when to pivot to M47.12, when to add M54.12, how to handle radiculopathy layered on top, and how all of this connects to related codes like lumbar stenosis ICD-10, lumbosacral stenosis ICD-10, and neural foraminal stenosis ICD-10.
In 2026, with increased payer scrutiny and evolving DRG grouping under MS-DRG v43.0, precision in spine coding is not optional. Every claim you submit tells a clinical story — and your ICD-10 codes need to tell that story clearly, specifically, and accurately.
About This Article: Written by a medical coding professional with over 10 years of experience in musculoskeletal and spine billing. All codes referenced are from the official 2026 ICD-10-CM edition, effective October 1, 2025. Always consult your payer-specific guidelines and CMS LCDs for jurisdiction-specific requirements.




