

If you’ve seen the code M54.16 on a patient chart, an insurance form, or your own medical paperwork and had no clue what it means, you’re definitely not alone. Every day, patients, medical billers, coders, chiropractors, physical therapists, and primary care docs deal with this code. And getting it wrong costs real money, delays treatment, and causes claim denials.
So let’s fix that right now.
This is your complete, 2026-updated guide to understanding what is M54.16, what is lumbar radiculopathy M54.16, how to diagnose it, how to bill it correctly, what mistakes to avoid, and what has changed this fiscal year. Whether you’re a patient trying to understand your paperwork or a coder trying to protect your reimbursement, this article covers everything you need, start to finish.
What Is M54.16? Breaking Down the Diagnosis Code
Let’s start at the very beginning because this matters.
M54.16 is an official ICD-10-CM diagnosis code. ICD-10-CM stands for International Classification of Diseases, 10th Revision, Clinical Modification. Every disease, condition, and injury a doctor can diagnose in the United States gets its own unique code in this system. Payers, hospitals, and government agencies use these codes to process claims, track health data, and determine reimbursement.
The full official name of M54.16 is Radiculopathy, Lumbar Region.
Now, before that sounds too clinical, here is what every single character in that code is actually telling you:
- M = This is a disease of the musculoskeletal system, meaning muscles, bones, joints, or connective tissue
- 54 = This falls under “Dorsopathies,” which is the umbrella term for back and spine conditions
- .1 = This is specifically radiculopathy, meaning a nerve root is irritated or compressed
- 6 = The number 6 identifies the lumbar region, meaning the lower back, spanning vertebrae L1 through L5
Think of the code like a street address for a medical problem. M54 gets you to the right neighborhood. The .1 takes you to the right street. The 6 puts you right at the doorstep. When a provider assigns M54.16, they are telling everyone involved, including the insurance company, that their patient has a compressed or irritated nerve root specifically in the lower back.
What Does Diagnosis Code M54.16 Mean for a Patient?
If you are a patient and someone just handed you paperwork with M54.16 on it, here is exactly what that means in plain English: your doctor has concluded that one or more of the nerve roots in your lower back are being pinched, squeezed, or irritated. That nerve problem is producing real, clinically significant symptoms, most commonly pain, numbness, tingling, or weakness that travels down into your hips, legs, or feet.
People often call this a “pinched nerve in the back.” The clinical community calls it lumbar radiculopathy. Both terms lead to the same code: M54.16 radiculopathy lumbar region. Your insurance company needs this code to understand what your provider treated, justify your care, and process your claim.
What Is Diagnosis M54.16 in the ICD Hierarchy?
Within the ICD-10-CM system, M54.16 sits inside these parent categories:
- Chapter M00-M99: Diseases of the musculoskeletal system and connective tissue
- Block M50-M54: Other dorsopathies
- Category M54: Dorsalgia (back pain)
- Subcategory M54.1: Radiculopathy
- Specific code M54.16: Radiculopathy, lumbar region
This structure matters for coders because parent codes like M54.1 are not billable by themselves. You always need to code down to the most specific level. M54.16 is a billable, specific code and it is valid for the entire 2026 fiscal year, running from October 1, 2025 through September 30, 2026.
What Is Lumbar Radiculopathy M54.16? The Clinical Picture
Now that you understand the code, let’s talk about the actual condition it represents.
What is lumbar radiculopathy M54.16 from a clinical standpoint? Lumbar radiculopathy happens when a nerve root exiting the spinal cord between vertebral levels L1 and S1 becomes compressed, inflamed, or irritated. Your lumbar spine carries the majority of your body’s daily load. Every time you sit, stand, bend, lift, or twist, those five vertebrae and the nerve roots branching off your spinal cord at those levels are working hard.
When something goes wrong in that region, whether it’s a disc that bulges out of place, a bone spur forming from arthritis, or a narrowed spinal canal, those nerve roots get caught in the crossfire. The nerve starts misfiring. And because these nerves carry signals all the way down your legs to your feet, the symptoms often show up far away from where the actual compression is happening.
This is one reason lumbar radiculopathy gets misdiagnosed or underappreciated. A patient says their foot hurts, or their calf burns. The actual problem is a pinched nerve in their lower back. The M54.16 diagnosis captures that connection precisely.
Symptoms of M54.16 Lumbar Radiculopathy
Knowing the symptoms of what is M54.16 helps providers document accurately and helps patients advocate for themselves. The symptom pattern in lumbar radiculopathy is distinctive and clinically recognizable.
Radiating Leg Pain (The Hallmark Symptom)
The defining feature of lumbar radiculopathy is pain that radiates from the lower back down through the buttock and into the leg. Patients describe it as sharp, burning, electric, shooting, or stabbing. Importantly, this pain typically travels past the knee, often reaching the calf, ankle, or foot.
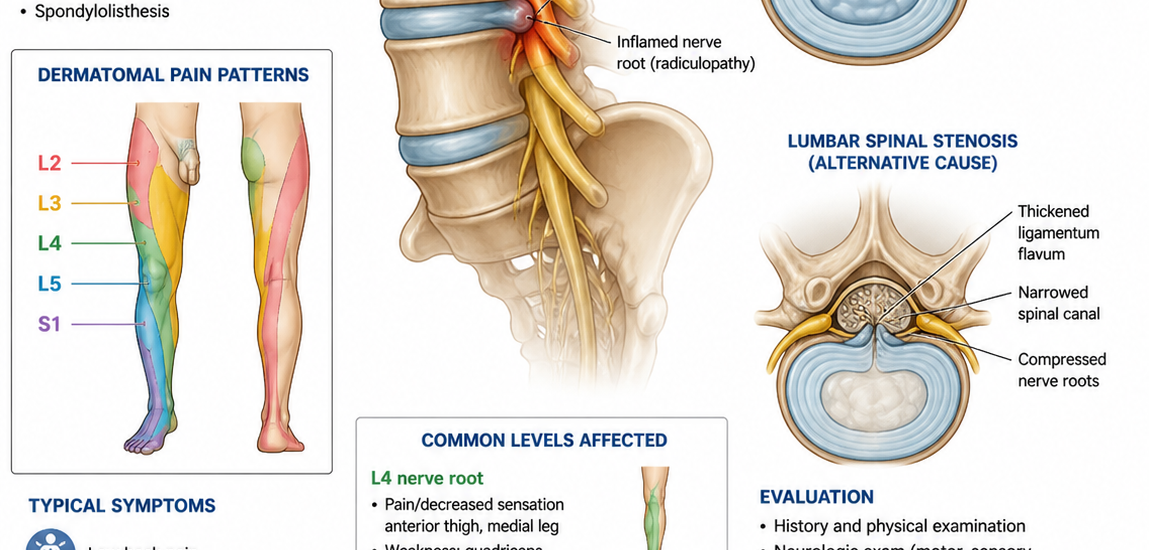
The location of that radiating pain gives skilled clinicians a strong clue about which nerve root is affected. Running down of pain in the front of the thigh into the knee typically suggests L3 or L4 involvement. Pain wrapping around the hip to the outside of the leg and into the big toe points toward L5. Pain shooting down the back of the leg into the heel and little toe suggests S1 compression.
When this pain follows the sciatic nerve pathway, people call it sciatica. And while sciatica is technically a symptom, not a separate diagnosis, it almost always signals underlying lumbar radiculopathy.
Numbness and Tingling
Beyond pain, nerve compression disrupts sensory signals. Most patients with M54.16 report patches of numbness, tingling, or that familiar “pins and needles” feeling in their leg or foot. These sensory changes follow a dermatomal pattern, meaning they occur in a predictable strip of skin that corresponds to the specific nerve root being compressed.
This dermatomal distribution is an important diagnostic clue. Random numbness anywhere in the leg does not confirm radiculopathy. Numbness that follows a precise nerve root territory does.
Muscle Weakness
When nerve compression is significant or has persisted for some time, the muscles supplied by that nerve root start to weaken. A patient with L4 compression might struggle to flex their foot upward. Someone with L5 involvement may notice their toes dragging when they walk. S1 compression weakens the push-off phase of walking and reduces calf strength.
Muscle weakness in lumbar radiculopathy is a red flag for more serious nerve damage. Providers who notice significant weakness on exam need to accelerate the diagnostic workup and consider urgent imaging.
Reflex Changes
Deep tendon reflexes are one of the most objective clinical findings in lumbar radiculopathy. The knee jerk reflex (patellar tendon reflex) depends heavily on the L4 nerve root. The ankle jerk reflex (Achilles tendon reflex) depends on S1. When a provider taps these tendons and gets a diminished or absent reflex on one side compared to the other, that finding supports a radiculopathy diagnosis and helps pinpoint which level is affected.
Positions That Make It Worse
Most patients with M54.16 notice that certain positions dramatically increase their symptoms. Sitting for extended periods is a common trigger. Forward bending, coughing, sneezing, or straining with a bowel movement can cause a sharp spike in leg pain. These aggravating factors happen because they increase pressure inside the spinal canal or around the affected nerve root.
On the flip side, lying down with the hips and knees slightly bent often brings temporary relief. Some patients find walking short distances more comfortable than sitting still.
Causes of M54.16 Lumbar Radiculopathy
Understanding the causes behind what is M54 16 radiculopathy gives both the clinical picture and the coding picture more depth. Several different structural problems can produce lumbar radiculopathy, and the underlying cause sometimes affects which ICD-10 code you should ultimately use.
Herniated Lumbar Disc
A herniated disc is by far the most common culprit, especially in patients between 30 and 50 years old. Spinal discs act as cushions between vertebrae. When the tough outer ring of a disc develops a tear, the softer inner material can push backward into the spinal canal, pressing directly on a nerve root. The resulting compression causes the classic M54.16 radiculopathy lumbar symptom pattern.
If imaging confirms that a herniated disc is the direct cause of the radiculopathy, the coding rules actually point you toward M51.16, which is the more specific code for intervertebral disc disorder with radiculopathy in the lumbar region. More on that in the related codes section.
Spinal Stenosis
Spinal stenosis means the spinal canal or the nerve exit tunnels (foramina) have narrowed. Bone spurs growing from arthritic changes, thickened ligaments, or a combination of both can gradually reduce the space where nerve roots live. As a result, the nerve roots get chronically compressed. This cause becomes increasingly common in adults over 60. Stenosis-related radiculopathy tends to develop slowly and often causes bilateral symptoms rather than the strictly one-sided pattern seen with disc herniation.
Degenerative Disc Disease
As the spine ages, discs naturally lose hydration and height. This gradual degeneration causes the vertebrae to settle closer together, which can close off the foraminal openings where nerve roots exit. Degenerative disc disease rarely causes a dramatic acute event, but it builds a structural environment where radiculopathy can develop over time.
Spondylolisthesis
Spondylolisthesis happens when one vertebra slips forward over the one below it. That forward migration can directly compress the nerve root exiting at that spinal level. It produces a characteristic radicular pain pattern that corresponds to the nerve root being pinched at the slip site.
Other Causes Worth Noting
Several less common causes also lead to an M54.16 diagnosis, including spinal cysts pressing on nerve roots, vertebral fractures from osteoporosis, diabetes-related nerve damage with radicular characteristics, tumor involvement near the spinal canal, and severe muscle spasms that secondarily compress nerve structures.
How Doctors Confirm a Diagnosis of M54.16
Proper documentation starts with a thorough diagnostic process. Providers cannot simply write M54.16 on a form because a patient has back pain. The diagnosis needs clinical support, and that support needs to show up clearly in the medical record.
Physical Examination
The straight leg raise test, also called Lasegue’s sign, is the workhorse exam for lumbar radiculopathy. The examiner slowly raises the patient’s straight leg off the table. When nerve root irritation is present, this maneuver reproduces radicular leg pain between 30 and 60 degrees of elevation. A positive result is one of the strongest clinical indicators that M54.16 applies.
The slump test adds another layer. The patient sits with neck flexed and extends one knee while staying slumped forward. Reproduction of the familiar radiating symptoms points toward nerve root involvement.
Beyond these provocative tests, the provider checks muscle strength in both legs, compares deep tendon reflexes side to side, maps out the patient’s sensory changes, and assesses their gait. All of these findings together build the clinical case for lumbar radiculopathy.
Imaging
MRI without contrast is the go-to imaging study for confirming M54.16 radiculopathy lumbar diagnoses. MRI shows the nerve roots, the discs, the ligaments, and the surrounding soft tissue with excellent detail. It clearly identifies disc herniation, canal narrowing, foraminal stenosis, and direct nerve root compression.
CT scanning works when MRI is not possible. Plain X-rays show bony structure and can reveal alignment problems, bone spurs, or signs of spondylolisthesis, but they cannot visualize nerve tissue directly.
Standard guidance suggests imaging becomes necessary when symptoms persist beyond four to six weeks despite conservative treatment, or when any red flags are present, including significant weakness, bowel or bladder changes, unexplained weight loss, or fever.
Electrodiagnostic Testing
EMG (electromyography) and nerve conduction studies provide functional data about how well the affected nerve is working. These tests become especially valuable when imaging results and clinical findings do not fully align, or when the provider needs to rule out peripheral neuropathy, which can mimic radiculopathy symptoms. They are also useful for documenting the severity and chronicity of nerve involvement.
M54.16 Billing Tips: Protect Your Revenue in 2026
This is where the rubber really meets the road for providers, coders, and billing staff. Getting M54.16 right protects your claims, speeds up reimbursement, and keeps you clear of audits. Here are the most practical tips for billing this code correctly in 2026.
Nail Your Documentation First
Everything starts with documentation. The clinical note must explicitly state that the diagnosis is radiculopathy in the lumbar region, not just “back pain” or “lower back discomfort.” The note needs to capture the patient’s specific symptoms, the physical exam findings that support the diagnosis including any positive provocative tests, and the imaging or diagnostic results that confirm nerve root involvement.
Vague documentation is the number one reason M54.16 claims get denied or audited. Specificity is not optional. Write the diagnosis clearly. Connect the findings to the diagnosis explicitly. Let the note tell the full story.
Choose the Right Code for the Right Situation
M54.16 applies when lumbar radiculopathy is the confirmed diagnosis and no more specific causative code is available or appropriate. However, if your patient has imaging-confirmed disc herniation causing the radiculopathy, M51.16 is the more precise code. Payers increasingly expect the highest level of coding specificity, and using M54.16 when M51.16 is warranted can trigger additional scrutiny.
Similarly, do not use M54.16 as a primary surgical code. If a patient is going to surgery for lumbar nerve root decompression, the surgical claim needs a cause-specific code like M51.16 or M48.06. Using M54.16 alone on a surgical claim will almost certainly result in a denial.
Always Address Laterality
M54.16 does not include information about which side of the body is affected. The code is silent on right versus left. For accurate claim submission, you need to add a separate laterality code specifying the affected side. Many coders miss this step. Do not be one of them. Check your billing platform’s options for adding right-sided or left-sided leg symptom codes alongside M54.16.
Know Your CPT Pairings
When billing services related to an M54.16 diagnosis, these CPT codes come up frequently and need to align with the documentation:
- 99213 / 99214: Established patient office visits at moderate or high complexity
- 72148: MRI of the lumbar spine without contrast
- 62322 / 62323: Lumbar interlaminar epidural steroid injections
- 64483: Lumbar transforaminal epidural injection
- 97110 / 97530: Physical therapy therapeutic exercises and activities
- 95886: EMG needle examination of extremity muscles
- 64493-64495: Facet joint nerve blocks if relevant
Pairing the right CPT codes with M54.16 and backing them up with clear medical necessity documentation is how you get paid on time, every time.
Understand Pre-Authorization Requirements
Basic conservative care, such as an initial course of physical therapy, generally does not require prior authorization from most payers. However, epidural steroid injections, advanced diagnostic imaging ordered after initial treatment, and surgical referrals typically need pre-approval. Skipping pre-authorization steps is an expensive mistake. Build a workflow that checks payer-specific pre-auth requirements for each service tied to an M54.16 diagnosis before scheduling the patient.
Match Treatment Intensity to Documented Severity
Payers in 2026 scrutinize whether the level of treatment intensity matches the documented severity of the condition. A patient with mild M54.16 symptoms being billed for repeated injections without documented failure of conservative care is a red flag for auditors. Build your documentation trail from the first visit. Record baseline severity, track functional limitations, document the patient’s response to each treatment step, and justify every escalation in care.
Related ICD-10 Codes for Lumbar Radiculopathy
Understanding the full neighborhood of codes around M54.16 helps you avoid costly coding errors and choose the right code for each clinical situation.
M54.10 – Radiculopathy, site unspecified Use this only when the location of the radiculopathy truly cannot be identified. This is rare in clinical practice and should not become a default code.
M54.12 – Radiculopathy, cervical region This is the equivalent code for nerve root compression in the neck causing arm pain. Do not confuse it with M54.16.
M54.14 – Radiculopathy, thoracic region Mid-back nerve root irritation. Uncommon compared to cervical and lumbar radiculopathy.
M54.17 – Radiculopathy, lumbosacral region This code applies when the radiculopathy involves the junction between the lumbar and sacral spine. It is closely related to M54.16 but distinct.
M51.16 – Intervertebral disc disorder with radiculopathy, lumbar region This is the more specific code when imaging confirms a herniated or degenerated disc is directly causing the radiculopathy. Many cases that start as M54.16 should transition to M51.16 once imaging results come back. Getting this distinction right matters significantly for reimbursement, especially for injection claims and surgical authorization.
M47.26 – Spondylosis with radiculopathy, lumbar region When arthritic spinal changes, specifically spondylosis, are the confirmed cause of the nerve root compression, this more specific code applies rather than M54.16.
M54.50 – Low back pain, unspecified This is the code for simple low back pain without nerve root involvement. It is completely different from M54.16. Never use these two codes interchangeably.
The most critical distinction to remember is between M54.16 and M51.16. Experienced coders treat imaging results as the tipping point. No confirmed disc cause, use M54.16. Confirmed disc pathology causing the radiculopathy, switch to M51.16.
Common Coding Mistakes with M54.16
Even seasoned coders and experienced providers make these errors. Here are the most common ones, along with how to avoid each of them.
Using M54.16 for General Low Back Pain
This is probably the most widespread mistake. M54.16 specifically requires nerve root involvement, meaning radiculopathy. A patient with localized low back pain who reports no leg symptoms, no dermatomal numbness, and no neurological signs does not have radiculopathy. Their diagnosis is low back pain, coded as M54.50 or M54.51. Using M54.16 for general back pain is technically inaccurate and opens the door to audit risk.
Ignoring Laterality
M54.16 does not encode which side is affected. Submitting claims without any laterality information leaves your documentation incomplete. Always add the appropriate side-specific code for the patient’s symptoms. This step takes thirty seconds and it protects your claim.
Keeping M54.16 After Imaging Confirms Disc Herniation
A lot of providers assign M54.16 at the first visit because imaging has not been done yet, which is totally appropriate. The mistake happens when they never update the code after MRI comes back confirming a herniated disc. Once disc herniation is documented as the cause, the correct code becomes M51.16. Failing to update the diagnosis code means you are coding less specifically than the clinical record supports.
Using M54.16 as a Primary Code for Surgical Claims
M54.16 alone cannot justify surgical intervention to an insurance company. Surgery for lumbar radiculopathy requires a cause-specific code like M51.16 or M48.06 to establish medical necessity. Sending a surgical claim with only M54.16 will almost certainly result in a denial.
Linking Services to the Wrong Diagnosis
Every procedure billed needs to tie directly back to the diagnosis code that justifies it. A common denial pattern occurs when providers bill physical therapy or injection codes alongside M54.16 but the clinical note does not explicitly connect the treatment to the radiculopathy diagnosis. The auditor reads the note, sees no clear link between the service and the nerve root problem, and denies the claim. Write the connection into your notes every time.
Confusing Sciatica Codes with M54.16
Sciatica (M54.3 series) and lumbar radiculopathy (M54.16) are related but they are separate code categories in ICD-10. Sciatica codes include laterality options (right, left, unspecified). Radiculopathy codes under M54.1 do not. If the provider’s documented diagnosis is radiculopathy with clinical confirmation of nerve root involvement, M54.16 is correct. If the provider documents sciatica as a symptom without confirming nerve root pathology, you stay in the M54.3 family.
2026 Updates: What Changed for M54.16 This Year
Medical coding is never static. Here is everything you need to know about what is current and relevant for M54.16 in 2026.
Code Validity for Fiscal Year 2026
The 2026 edition of ICD-10-CM officially became effective on October 1, 2025. M54.16 remains a valid, billable, and specific code throughout the current fiscal year, covering all HIPAA-compliant claim submissions through September 30, 2026. No changes were made to the code’s definition or its official description in this revision cycle.
All claims with a service date on or after October 1, 2015, must use ICD-10-CM codes. The older ICD-9 system is obsolete. Any practice still referencing ICD-9 crosswalk data for M54.16 should note that the approximate legacy equivalent was 724.4, but that code is no longer acceptable for any current submission.
CMS Administrative Simplification Final Rule, March 2026
In March 2026, the Centers for Medicare and Medicaid Services finalized its Administrative Simplification rule, adopting updated electronic data exchange standards for healthcare claims. This rule directly affects how practices submit claims electronically for codes including M54.16. Practices need to verify that their billing and practice management software platforms are fully compliant with these updated electronic transaction standards before submitting claims to Medicare or Medicaid.
Medicaid Funding Rule Changes, April 2026
The April 2026 Medicaid final rule introduced structural changes to how state Medicaid programs are funded, specifically targeting provider tax arrangements. Practices that treat a significant volume of Medicaid patients for musculoskeletal conditions, including lumbar radiculopathy, should review how these funding changes affect their local Medicaid reimbursement rates and contract terms. This is especially relevant for physical therapy practices, chiropractic offices, and pain management clinics where M54.16 appears frequently on claim submissions.
MS-DRG Grouper Version 43.0
For inpatient hospital billing, M54.16 falls under MS-DRG Version 43.0, applicable from October 1, 2025, through September 30, 2026. Specifically, M54.16 groups into:
- DRG 551: Medical back problems with major complication or comorbidity (MCC)
- DRG 552: Medical back problems without MCC
The DRG assigned directly affects the base payment rate for inpatient hospital stays where lumbar radiculopathy is the principal diagnosis. Accurate capture of comorbidities matters here because the difference between DRG 551 and 552 is financially significant.
AI Documentation Tools and Coding Compliance
A growing number of practices in 2026 use AI-assisted documentation tools that can auto-suggest ICD-10 codes, including M54.16, based on transcribed clinical notes. These tools can dramatically speed up workflow and reduce documentation gaps. However, providers must still review every AI-suggested code against the actual clinical findings. An AI tool that sees “lower back pain with leg symptoms” in a note might suggest M54.16, but the provider needs to confirm that the documented findings genuinely support a radiculopathy diagnosis before submitting that code. The provider, not the software, remains responsible for coding accuracy.
Conservative First, Then Escalate: Payer Trends in 2026
Major payers in 2026 continue reinforcing conservative-care-first policies for M54.16 diagnoses. Before approving epidural steroid injections, most insurers now require documented evidence of a six-to-eight week trial of conservative treatment, including physical therapy, activity modification, and at least one anti-inflammatory medication trial. Building this documentation trail from the patient’s first visit is not optional. It is what unlocks access to higher-level interventions when conservative care does not deliver adequate relief.
Treatment Approaches for Lumbar Radiculopathy
While this guide focuses primarily on the coding and clinical understanding of M54.16, a practical overview of treatment helps providers document the care continuum correctly and helps patients understand their road ahead.
Conservative Care: The Starting Point
Most guidelines and payers agree that conservative management comes first for M54.16 radiculopathy lumbar presentations. This typically includes a structured physical therapy program incorporating nerve gliding exercises, core strengthening, postural correction, and McKenzie method techniques. Anti-inflammatory medications help reduce nerve root swelling, and activity modifications protect the spine from positions that aggravate symptoms.
Most patients with lumbar radiculopathy see meaningful improvement within six to twelve weeks of consistent conservative care. This is why payers require it before approving escalation.
Interventional Pain Management
When conservative care does not provide sufficient relief after six to eight weeks, interventional options become appropriate. Epidural steroid injections deliver anti-inflammatory medication directly around the compressed nerve root, reducing swelling and providing pain relief that lets patients engage more effectively in physical therapy. Transforaminal approaches target a specific nerve root level with greater precision than interlaminar approaches.
These injections often provide weeks to months of significant symptom relief, and the documentation of their use ties directly back to the M54.16 diagnosis code throughout the claim submission process.
Surgical Intervention
Surgery becomes appropriate for a minority of M54.16 patients, specifically those with significant weakness, bowel or bladder involvement, intolerable pain despite exhausting conservative and interventional options, or progressive neurological deterioration. Surgical options include microdiscectomy for disc herniation and various decompression procedures for stenosis. At the surgical coding stage, M54.16 transitions to more specific cause-based codes.
Frequently Asked Questions About M54.16
What is lumbar radiculopathy M54.16 in simple terms?
M54.16 is the official medical code for a pinched or irritated nerve root in the lower back. The condition produces pain, numbness, tingling, or weakness that typically travels from the lower spine down through the leg. Doctors, hospitals, and insurance companies use this code to identify the diagnosis and process billing.
What does diagnosis code M54.16 mean on my medical paperwork?
It means your healthcare provider has diagnosed you with radiculopathy in the lumbar region of your spine. In everyday language, one or more nerve roots in your lower back are being compressed or irritated, causing symptoms that radiate into your legs.
What is M54.16 and how is it different from back pain?
M54.16 specifically means nerve root involvement in the lower back, not just general back pain. A person with simple low back pain that stays in the back uses a completely different diagnosis code. M54.16 only applies when nerve root compression produces radiating symptoms into the legs.
Is M54.16 the same as sciatica?
Not exactly, though they are closely related. Sciatica is a symptom involving pain along the sciatic nerve’s path down the leg. Lumbar radiculopathy is the diagnosis explaining why that symptom exists. M54.16 and sciatica codes are separate within ICD-10-CM.
What is the difference between M54.16 and M51.16?
M54.16 is used when lumbar radiculopathy is confirmed but no specific disc pathology has been identified as the cause. M51.16 is the more specific code used when imaging confirms that an intervertebral disc disorder is directly causing the radiculopathy. When disc herniation is documented, M51.16 is the preferred code.
Can a physical therapist or chiropractor use M54.16?
Yes. Licensed physical therapists, chiropractors, physiatrists, and other qualified healthcare providers can use M54.16 as a diagnosis code when their clinical findings support lumbar radiculopathy. The code is not restricted to physicians alone.
How long does it take to recover from lumbar radiculopathy?
Most people with an M54.16 diagnosis show meaningful improvement within six to twelve weeks with appropriate conservative care including physical therapy and anti-inflammatory treatment. A smaller subset needs interventional procedures. A very small minority requires surgery.
Does M54.16 require an MRI to be valid for billing?
No. MRI is not required before assigning or billing M54.16. Clinical diagnosis based on history, physical exam findings, and provocative testing is sufficient to assign the code. However, MRI is strongly recommended when symptoms persist beyond four to six weeks or when red flags appear.
What happens if I use the wrong code instead of M54.16?
Using the wrong code can result in claim denials, delayed reimbursement, payer audits, and potential compliance issues. For example, using M54.50 (general low back pain) instead of M54.16 when radiculopathy is clearly documented understates the clinical complexity and typically results in lower reimbursement for associated services.
Final Word: Why Getting M54.16 Right Matters in 2026
Lumbar radiculopathy is one of the most common musculoskeletal diagnoses in the United States. Low back conditions collectively account for tens of billions of dollars in healthcare spending each year, and conditions coded under M54.16 make up a significant slice of that volume. When this code gets used accurately, it drives correct treatment decisions, appropriate reimbursement, and clean claims. When it gets used sloppily, it costs practices money, delays patient care, and creates compliance headaches.
For patients, understanding what is diagnosis M54.16 empowers you to ask better questions, understand your treatment plan, and communicate more clearly with your care team. For providers and coders, applying everything in this guide means your documentation tells the right clinical story, your claims go through cleanly, and your patients get access to the care they need without unnecessary insurance friction.
The code is simple. The condition behind it is complex, real, and genuinely disabling for the people who live with it. Treat both with the seriousness they deserve.
This article reflects current ICD-10-CM guidelines and clinical coding standards for fiscal year 2026 (October 1, 2025 through September 30, 2026). Always consult your payer-specific policies and a certified coding professional for practice-specific guidance.
Focus Keyword: M54.16 Slug: what-is-m54-16-lumbar-radiculopathy-diagnosis-code-explained Meta Title: M54.16: What Is Lumbar Radiculopathy? Full 2026 Guide Meta Description: Learn what M54.16 means, its symptoms, causes, billing tips, related codes & 2026 updates for lumbar radiculopathy diagnosis.




