

If you’ve ever looked at a medical bill or an explanation of benefits and wondered, what does M54.9 diagnosis code mean — you’re definitely not alone. Millions of Americans deal with back pain every single year, and this particular code shows up on claims, patient records, and insurance paperwork more often than almost any other musculoskeletal diagnosis in the country. So, let’s break it all down in plain English — no confusing jargon, no runaround.
Whether you’re a patient trying to decode your paperwork, a medical coder looking for clarity, or a provider brushing up on the 2026 ICD-10-CM guidelines, this guide covers everything you need to know about M54.9.
What Is M54.9 diagnosis code?
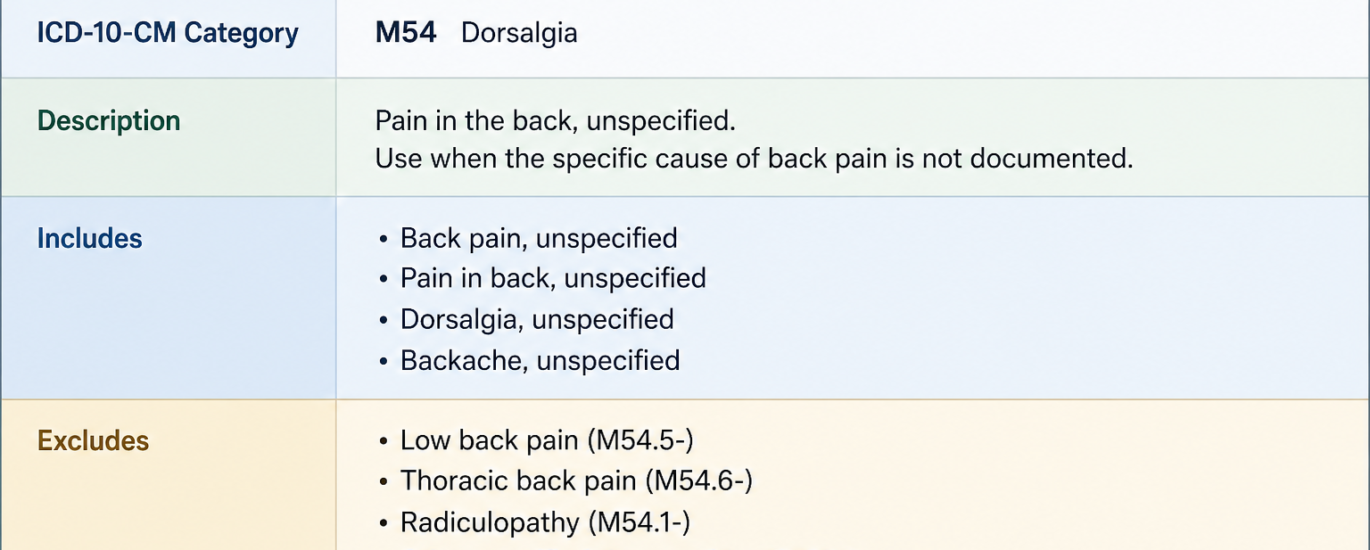
So, what is M54.9? Simply put, M54.9 is the ICD-10-CM diagnosis code for Dorsalgia, Unspecified. The word “dorsalgia” comes from two Latin roots: dorso, meaning back, and algia, meaning pain. Put them together, and you’ve got back pain — plain and simple.
The word “unspecified” is the key part here. It tells payers, insurers, and anyone reading the record that the patient has back pain, but the clinical documentation doesn’t pinpoint exactly where in the spine the pain is coming from — or what’s causing it.
In practical terms, what is diagnosis code M54.9 telling a payer? It’s saying: “This person has back pain, but we don’t have enough clinical detail to call it lumbar, thoracic, cervical, or anything more specific right now.”
The official ICD-10-CM description also recognizes M54.9 under two synonyms:
- Backache NOS (Not Otherwise Specified)
- Back Pain NOS
Both of these labels confirm the same thing — the pain is real, it’s documented, but the region or root cause hasn’t been nailed down in the chart yet.
Where Does M54.9 Fit in the ICD-10-CM Structure?
M54.9 sits inside a very clear hierarchy within the ICD-10-CM system:
- Chapter 13 — Diseases of the Musculoskeletal System and Connective Tissue (M00–M99)
- Block M50–M54 — Other Dorsopathies
- Category M54 — Dorsalgia
- Code M54.9 — Dorsalgia, Unspecified
This code is maintained by the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). It became effective for billing on October 1, 2015, and remains fully active in the FY2026 code set (October 1, 2025 through September 30, 2026) with no modifications.
Symptoms Associated With Diagnosis Code M54.9
Now, here’s where things get real for the patient side of this equation. When a provider assigns M54.9 to your visit, they’re typically documenting one or more of the following symptoms:
Common Symptoms Linked to M54.9
- Diffuse or generalized back pain that doesn’t clearly localize to a single region of the spine
- Dull, aching discomfort felt across the upper, middle, or lower back without a specific pattern
- Stiffness in the back, especially in the morning or after long periods of sitting
- Pain that worsens with movement, bending, lifting, or prolonged standing
- Muscle tension or tightness along the paraspinal muscles on either side of the spine
- Radiating discomfort to the ribs, hips, or buttocks without a clear nerve-specific pattern
- Pain that fluctuates between acute flares and periods of relative relief
Importantly, M54.9 doesn’t apply when the provider has clearly identified the source — like a herniated disc, a vertebral fracture, or a nerve compression issue. In those cases, more specific codes take over. M54.9 is the code that fits when the clinical picture is still being pieced together or when the back pain is genuinely nonspecific.
What Causes Back Pain Coded Under M54.9?
Because M54.9 is an unspecified code by definition, the causes it represents are broad. However, clinical patterns consistently show up in patients who carry this code. Here are the most common ones:
Muscle Strain and Overuse
This is probably the number one driver behind M54.9 encounters. Improper lifting, sudden awkward movements, or simply doing too much physical activity can strain the paraspinal muscles. The pain is real, it’s documented, but early in the visit there may not be enough imaging or examination findings to point to a specific spinal structure.
Poor Posture and Sedentary Lifestyle
America’s growing desk-job culture has made postural back pain extremely common. Spending hours hunched over a screen creates chronic muscle tension across the entire spine — upper, mid, and lower. Because the pain is spread out and not region-specific, providers often default to M54.9 at the initial encounter.
Stress and Psychological Factors
Yes, stress genuinely causes physical back pain. Chronic stress leads to muscle tension, disrupted sleep, and altered pain perception — all of which contribute to generalized back discomfort that doesn’t neatly fit into a specific anatomical bucket.
Age-Related Degenerative Changes
As people get older, the discs and joints in the spine naturally wear down. Early-stage degeneration may produce diffuse back pain before imaging reveals anything conclusive enough to code more specifically.
Obesity and Physical Deconditioning
Excess body weight puts a tremendous load on the entire spinal column, not just the lumbar region. Combined with weak core muscles, this produces generalized back pain that fits the M54.9 description well.
Undocumented or Unknown Etiology
Sometimes, the honest answer is that the provider simply doesn’t know yet. Maybe the patient is on their first visit. Maybe the imaging is pending. In these situations, M54.9 is the medically and ethically correct code to assign — because it reflects exactly what is known at that moment.
M54.9 Billing Tips: Getting Claims Right in 2026
Here’s where medical billers, coders, and practice managers need to pay close attention. M54.9 is a billable and specific ICD-10-CM code, which means it goes directly on the claim. However, billing it incorrectly — or leaning on it too heavily — creates real financial and compliance problems.
When It’s Appropriate to Use M54.9
Use M54.9 when:
- The provider’s documentation says “back pain” without specifying lumbar, thoracic, or cervical
- Pain involves multiple spinal regions without a dominant area identified
- It’s an initial encounter and imaging or workup hasn’t established a more specific diagnosis
- The clinical record doesn’t contain enough detail to justify a more precise code
When You Should NOT Use M54.9
Avoid M54.9 when:
- The note specifies “low back pain” or “lumbar pain” — that’s M54.50, not M54.9
- The chart documents “thoracic spine pain” — code M54.A6 (or M54.6 depending on your system’s update status)
- Imaging confirms a disc herniation, spondylosis, or radiculopathy — more specific codes apply
- The pain is clearly cervicogenic — M54.2 is the right choice
CPT Codes Commonly Paired With M54.9
Pairing the wrong CPT code with M54.9 is one of the fastest ways to trigger a denial. Here are common pairings that typically pass payer review:
- 99202–99215 — Evaluation and management (E/M) office visits (new and established patients)
- 97110 — Therapeutic exercises targeting strength, endurance, flexibility, and range of motion
- 97140 — Manual therapy techniques including mobilization and traction
- 97530 — Therapeutic activities for functional improvement
- 72100 — Radiologic exam of the lumbar spine (when imaging is warranted)
Always ensure that the CPT code you’re billing logically connects to the M54.9 diagnosis. Billing for an MRI under M54.9 without proper medical necessity documentation is one of the most common denial triggers in 2026.
Does Medicare Pay for M54.9?
This question comes up constantly, so let’s address it head-on. Does Medicare pay for M54.9? The short answer is yes — M54.9 is a recognized, billable diagnosis code and Medicare does reimburse for services tied to it, as long as medical necessity is documented.
However, there are important caveats. Traditional Medicare and Medicare Advantage plans are tightening their stance on unspecified codes. If your practice is submitting M54.9 on a large portion of back pain claims, that pattern signals weak clinical documentation to payer reviewers. It can trigger medical record audits and delayed reimbursements.
Additionally, for Medicare’s covered acupuncture benefit for chronic low back pain, M54.9 alone typically does not qualify. Medicare’s acupuncture NCD specifically references codes like M54.50 and M54.59 for that benefit. So if you’re billing acupuncture under M54.9, expect a denial.
Related ICD-10 Codes You Should Know
Understanding where M54.9 diagnosis code sits among its neighbors helps you avoid coding the wrong one. Here are the most important related codes:
| Code | Description | When to Use |
|---|---|---|
| M54.50 | Low back pain, unspecified | Documented lumbar or lower back pain |
| M54.51 | Vertebrogenic low back pain | Imaging-confirmed Modic changes or vertebral endplate damage |
| M54.59 | Other low back pain | Pain characteristics documented beyond just location |
| M54.2 | Cervicalgia | Neck/cervical spine pain |
| M54.A6 | Thoracic spine pain (2026 update) | Mid-back pain, thoracic region specified |
| M54.89 | Other dorsalgia | Specified back pain not fitting other subcategories |
| G89.29 | Other chronic pain | Used as secondary code alongside site-specific M54.5x for chronic pain |
Knowing these distinctions cold is what separates a solid coder from one who triggers constant claim scrubs.
Common Coding Mistakes With M54.9
After 10+ years of watching billing errors repeat themselves, these are the mistakes that show up again and again with M54.9:
Mistake 1: Using M54.9 When M54.50 Is Clearly Indicated
This is the single most common error. If the provider writes “low back pain” anywhere in the note — even just once — the correct code is M54.50. Defaulting to M54.9 when the region is documented is undercoding, and it’s a compliance risk.
Mistake 2: Never Updating the Code After New Findings Arrive
M54.9 is perfectly valid for an initial visit where information is incomplete. However, many practices forget to update the code when imaging results come in or when the next visit produces a clearer clinical picture. Stale codes on follow-up claims invite payer scrutiny.
Mistake 3: Over-Relying on M54.9 Across the Practice
A handful of M54.9 claims per month is totally normal. But when a significant percentage of your back pain encounters carry this code, payers see it as a documentation quality problem — not just an individual coding choice. That pattern can trigger a broader audit.
Mistake 4: Mismatching CPT and ICD Codes
Billing a spinal injection CPT code against M54.9 without rock-solid medical necessity documentation is a textbook denial. The diagnosis needs to logically support the service being billed, every single time.
Mistake 5: Submitting M54.5 (the Retired Code)
M54.5 was officially retired by CMS in October 2021. If your EHR still has it as an option and someone selects it, the claim auto-denies. Make sure your system is updated to the current M54.50, M54.51, and M54.59 options.
2026 Updates: What’s Changed for M54.9 diagnosis code and Related Codes
The FY2026 ICD-10-CM code set became effective on October 1, 2025, with a mid-year update applied on April 1, 2026. Here’s what matters for M54.9 diagnosis code specifically:
M54.9 Itself: No Changes
M54.9 is unchanged in FY2026. It carries the same description, the same billable status, and the same applicable-to notes it’s had since 2015. There are no new excludes notes or additional guidelines specific to this code for 2026.
The M54.A6 Shift for Thoracic Pain
This is a big one many coders are still catching up on. The 2026 coding landscape increasingly references M54.A6 as the preferred code for non-specific thoracic spine pain. While M54.6 (Pain in Thoracic Spine) hasn’t been officially retired, several payer LCDs and coding commentary now favor M54.A6 for mid-back pain without a structural cause. If you’re coding thoracic pain and previously defaulting to M54.9 because the note said “back pain, thoracic area,” check whether M54.A6 applies — it’s a more specific option.
Payer Scrutiny on Unspecified Codes Is Increasing
Across the board, commercial payers and Medicare Advantage plans are ramping up their review of unspecified diagnosis codes. The industry trend in 2026 is clear: specificity equals faster reimbursement. Unspecified codes aren’t invalid, but they’re receiving more pre-payment review than they were even two years ago. The fix is provider education and better documentation habits upstream — not a coding workaround downstream.
Documentation Requirements Are Getting Stricter
CMS’s emphasis on medical necessity documentation continues to intensify in 2026. For M54.9 specifically, claims without clear symptom onset, pain characteristics, examination findings, and treatment rationale are facing longer processing times and higher denial rates. Every M54.9 claim should be backed by clinical notes that explain why a more specific code wasn’t selected.
How to Avoid Claim Denials With M54.9 in 2026
Here’s a practical denial-prevention checklist that works:
- Query your providers when notes say “back pain” without a spinal region — a quick clarification note changes the code and saves the claim.
- Audit your code mix quarterly. If M54.9 diagnosis code represents more than 20–25% of your total back pain claims, that’s a red flag worth addressing.
- Train front-line coders on the M54.9 vs. M54.50 distinction — it’s the most common single-code decision in musculoskeletal billing.
- Update codes at each visit as new clinical information becomes available.
- Verify payer-specific LCDs before pairing M54.9 with high-dollar CPT codes like MRI or injections.
- Never submit M54.5 — it was retired in 2021 and guarantees an automatic denial.
Frequently Asked Questions About M54.9
What does M54.9 diagnosis code mean?
M54.9 means Dorsalgia, Unspecified — in everyday language, back pain that hasn’t been tied to a specific region of the spine or a specific cause in the clinical documentation.
What is M54.9 used for in medical billing?
Providers use it when a patient has back pain but the chart doesn’t have enough detail to support a more specific code. It’s a valid, billable ICD-10-CM code accepted by Medicare and most private insurers when properly documented.
What is the difference between M54.9 and M54.50?
M54.50 is for low back pain specifically tied to the lumbar region. M54.9 is for back pain without any regional specification at all. If the note says “low back pain,” use M54.50 — not M54.9.
Does Medicare pay for M54.9?
Yes, Medicare does reimburse services tied to M54.9, provided medical necessity is documented. However, M54.9 alone does not qualify for Medicare’s acupuncture benefit for chronic low back pain, which requires M54.50 or M54.59.
Is M54.9 a valid code in 2026?
Absolutely. M54.9 is fully active in the FY2026 ICD-10-CM code set (October 1, 2025 through September 30, 2026) with no changes from the prior year.
Can M54.9 be the primary diagnosis on a claim?
Yes. M54.9 can function as a principal or first-listed diagnosis when back pain is the primary reason for the encounter and no more specific condition has been identified.
What CPT codes pair with M54.9?
Common pairings include E/M codes (99202–99215), physical therapy codes (97110, 97140, 97530), and diagnostic imaging codes when medical necessity is clearly supported.
Why would a doctor write M54.9 on my records?
Most likely because you described back pain at your visit but didn’t have imaging or examination findings that pointed specifically to the lumbar, thoracic, or cervical spine. It’s a common, legitimate starting point for a back pain diagnosis.
The Bottom Line on M54.9 Diagnosis Code
M54.9 diagnosis code is one of the most used — and most misused — codes in the entire ICD-10-CM system. Understanding what it means, when to use it, and how to bill it correctly makes a real difference for both patient care documentation and practice revenue.
For patients, seeing M54.9 diagnosis code on your paperwork isn’t alarming. It simply means your provider documented your back pain and used the appropriate code based on the information available at that visit.
For providers and coders, the key takeaway is this: M54.9 is a legitimate code, but specificity always wins in 2026. The more detail that goes into the clinical note, the more specific — and more defensible — the code becomes. Use M54.9 when it’s genuinely the right choice, query providers when more detail is available, and update codes as the clinical picture sharpens.
Back pain touches more than 8 out of 10 Americans at some point in their lives. Coding it accurately is how the healthcare system tracks it, treats it, and gets paid for treating it right.




