E78.5 ICD-10 Code: Everything Coders and Billers Must Know in 2026
Let’s get right to it. The E78.5 ICD 10 code stands for “Hyperlipidemia, unspecified.” It is one of the most frequently billed diagnosis codes across primary care, internal medicine, endocrinology, and cardiology in the United States, and it also ranks among the most frequently misused. Providers, coders, and billing teams reach for this code every day, sometimes correctly, and sometimes when a more specific code would protect the claim far better.
The 2026 edition of E78.5 ICD 10 took effect on October 1, 2025, and stays valid for all HIPAA-covered transactions through September 30, 2026. It sits inside Chapter 4 of the ICD-10-CM system, which covers endocrine, nutritional, and metabolic diseases, specifically under category E78, the parent category for all disorders of lipoprotein metabolism and other lipidemias.
Using this code correctly does more than just pass a claim. It determines reimbursement accuracy, risk adjustment scores, audit vulnerability, and the quality of the clinical picture your documentation paints for payers and reviewers. Using it incorrectly, especially when a more specific code fits the documented facts, invites denials, downcoding, and costly post-payment audits.
What Is Hyperlipidemia and Why Does It Need a Code?
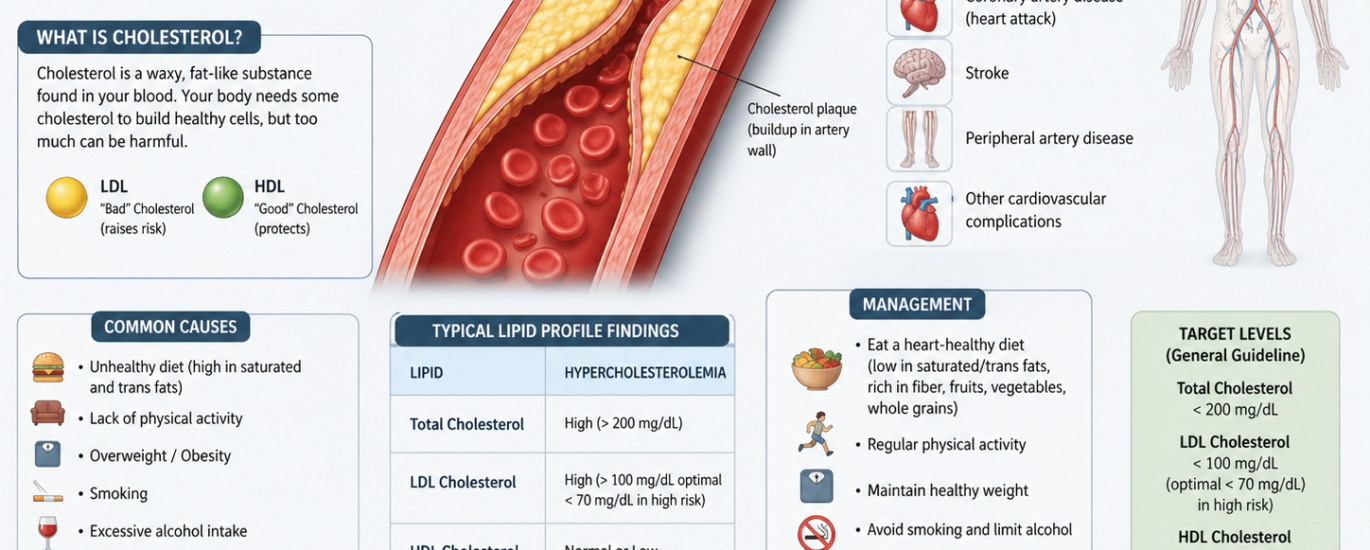
Before digging into the coding details, let’s build a solid clinical foundation. Hyperlipidemia is an umbrella term that describes abnormally elevated levels of lipids in the bloodstream. Lipids include cholesterol, triglycerides, and the lipoproteins that carry them through the blood. When any of these components rise above healthy reference ranges, the condition earns the label hyperlipidemia, and the clinical consequences can turn serious over time.
The most dangerous downstream effect of untreated hyperlipidemia is atherosclerosis, the slow buildup of fatty plaques along arterial walls. As these plaques grow, they narrow arteries, reduce blood flow, and dramatically raise the risk of heart attack, stroke, and peripheral artery disease. Cardiovascular disease remains the leading cause of death in the United States, and unmanaged lipid levels fuel that statistic directly.
Importantly, hyperlipidemia often shows zero symptoms in the early stages. The condition moves silently through the body for years, which is exactly why routine fasting lipid panels play such a critical role in early detection. When a lipid panel reveals elevated values, the provider must document the findings precisely, because that documentation determines which hyperlipidemia ICD 10 code fits the clinical picture.
When Should You Actually Use the E78.5 Diagnosis Code?
Here is where many practices go wrong: they treat E78.5 as a default code for any patient with a lipid problem, regardless of what the lab results and provider notes say. That habit creates real compliance exposure. The E78.5 diagnosis code belongs in your coding toolkit for specific situations only.
Use E78.5 when the provider documents hyperlipidemia, elevated lipids, or dyslipidemia without specifying whether the problem involves cholesterol, triglycerides, or both. In practical terms, reach for E78.5 in the following scenarios:
Initial visits with pending labs: When a patient presents at a first encounter, the provider suspects a lipid disorder based on family history or clinical signs, but the lipid panel results have not yet come back. The provider documents “hyperlipidemia” or “dyslipidemia” as a working diagnosis. E78.5 bridges the gap until more specific data arrives.
Documentation without lipid-type specificity: When the provider writes “hyperlipidemia” in the assessment without noting whether LDL, triglycerides, or both drive the abnormality, and the lipid panel results do not appear in the record to clarify, E78.5 fits the documented picture.
Transferred records with incomplete history: When a patient transfers from another practice and the incoming records reference a history of hyperlipidemia without specifying the type, E78.5 represents what the documentation actually supports until additional testing clarifies the picture.
The critical rule to remember: once a lipid panel confirms the specific type of lipid elevation and the provider documents it in the assessment, update the code. E78.5 should function as a temporary placeholder, not a permanent fixture on the problem list.
E78.5 vs E78.2: The Comparison Every Coder Gets Asked About
The E78.5 vs E78.2 question comes up constantly in coding forums, compliance discussions, and payer audits. Let’s break it down once and for all.
E78.5 — Hyperlipidemia, Unspecified Use this when the provider documents elevated lipids without identifying whether cholesterol, triglycerides, or a combination causes the problem. The word “unspecified” in the code title tells you everything: the clinical picture lacks the specificity to support a more precise code. E78.5 is a legitimate code when the documentation genuinely cannot support anything more specific, but it should never replace a specific code when the documentation clearly identifies the lipid type.
E78.2 — Mixed Hyperlipidemia Use this when both LDL cholesterol and triglycerides show elevations simultaneously and the provider documents both. E78.2 describes a dual-lipid problem, which is far more specific than the unspecified label that E78.5 carries. This code also typically shows up in cardiovascular risk discussions because the combination of elevated cholesterol and elevated triglycerides ICD 10 creates a compounded threat to arterial health.
The bottom line on E78.5 vs E78.2: if the lipid panel confirms both elevated cholesterol and elevated triglycerides, and the provider’s assessment reflects that, E78.2 is the correct code. Assigning E78.5 in that scenario under-codes the visit and leaves reimbursement and clinical accuracy behind. Many payers, including Medicare and major commercial plans, actively flag overuse of E78.5 when records clearly support more specific codes.
The Full E78 Code Family: Choosing the Right Code Every Time
Mastering the dx code E78.5 requires understanding how it fits within the broader E78 category. Here is a complete side-by-side breakdown.
E78.00 — Pure Hypercholesterolemia, Unspecified
Use this when the provider documents elevated LDL cholesterol specifically, with triglycerides staying within normal range. This is the classic hypercholesterolemia ICD 10 code. The ICD code for high cholesterol that primary care and cardiology practices use most frequently for straightforward high LDL cases is E78.00. Always choose E78.00 over E78.5 when the documentation confirms that only cholesterol, not triglycerides, runs high.
E78.01 — Familial Hypercholesterolemia
This subcode covers genetically inherited high cholesterol where a defective LDL receptor gene drives dramatically elevated LDL levels. When genetic testing confirms the familial type, or when the provider documents a clear family pattern of premature cardiovascular disease alongside very high LDL, E78.01 and its subcodes (E78.010 for homozygous, E78.011 for heterozygous) replace E78.00. Never use E78.5 when familial hypercholesterolemia is clearly documented.
E78.1 — Pure Hypertriglyceridemia
This code applies when only triglycerides ICD 10 runs above normal while cholesterol remains within range. Elevated triglycerides often reflect dietary patterns, alcohol use, uncontrolled diabetes, or genetic factors. When the provider documents isolated high triglycerides, E78.1 takes precedence over E78.5.
E78.2 — Mixed Hyperlipidemia
As covered above, E78.2 covers the dual-elevation scenario where both cholesterol and triglycerides run high together. This code carries stronger medical necessity support than E78.5 and passes through payer systems more cleanly because it reflects a specific, documented clinical condition.
E78.41 — Elevated Lipoprotein(a)
This newer, more specific code targets elevated Lp(a), an independent cardiovascular risk factor that standard lipid panels often miss. When a provider orders an Lp(a) test and documents elevation, E78.41 captures that specificity far better than E78.5.
E78.49 — Other Hyperlipidemia
Use this when the provider documents a specific lipid disorder that does not fit neatly into E78.00 through E78.41, such as non-HDL cholesterol elevation as a primary concern. This code captures documented specificity that falls outside the main subcategories.
E78.5 — Hyperlipidemia, Unspecified
After reviewing all the more specific options, E78.5 earns its place only when none of the above codes fits because the documentation genuinely lacks specificity. It is a legitimate last resort, not a first instinct.
Critical Billing Rules for the E78.5 ICD-10 Code
Getting claims through cleanly requires more than knowing which code to assign. These billing rules directly protect your reimbursement and compliance posture.
Never Code from Lab Values Alone
A lipid panel showing high LDL or elevated triglycerides does not automatically justify any E78 code. The provider must explicitly document a diagnosis in the assessment or problem list. A lab result sitting in the results section of the chart without a corresponding provider statement in the assessment does not support billing E78.5 or any other E78 code. Always locate the provider’s documented diagnosis before assigning the code.
Update E78.5 When Specific Information Becomes Available
When a provider initially assigns E78.5 because lab results are pending, the coder should flag that encounter for follow-up. Once the lipid panel results arrive and the provider documents the specific type of elevation, update the code to the most precise option. Leaving E78.5 on the problem list indefinitely when the record now supports a specific code creates audit risk and misrepresents the patient’s clinical status on future claims.
Payers Scrutinize E78.5 Overuse Heavily
Medicare, Blue Cross Blue Shield, Aetna, and other major payers actively track the volume of E78.5 codes across provider claims. When a practice submits E78.5 on nearly every lipid-related encounter regardless of what the documentation says, it signals to payers that documentation processes may not support the code selection. This pattern frequently triggers focused audits. Keep your E78.5 usage proportionate to genuine unspecified situations.
Pair E78.5 with the Correct Companion Codes
When E78.5 appears on a claim because the condition genuinely is unspecified at that encounter, add companion codes that strengthen the clinical picture:
Z79.899 — Other long-term (current) drug therapy: When the patient takes statins or fibrates on an ongoing basis for lipid management, this code documents active treatment and supports medical necessity for follow-up visits.
E11.65 — Type 2 diabetes with hyperglycemia: When diabetes contributes to or coexists with elevated lipid levels, code both conditions. Hyperlipidemia accelerates cardiovascular risk in diabetic patients, and payers expect to see both documented together.
I10 — Essential (primary) hypertension: When hypertension coexists with hyperlipidemia, which is extremely common in cardiometabolic patients, document both conditions. This combination strengthens the Hierarchical Condition Category (HCC) risk score, which affects value-based care reimbursement.
Z13.220 — Encounter for screening for lipoid disorders: Use this code instead of E78.5 when the lipid panel represents a screening test for an asymptomatic patient with no confirmed diagnosis. Never use E78.5 for a screening visit without a confirmed diagnosis supporting it.
Cloned Documentation Triggers Audits
One of the most dangerous billing habits in lipid disorder coding involves copying and pasting the same note from visit to visit without updating the lipid values, medication status, or clinical response. Auditors flag this as “cloned documentation,” and it leads to downcoding and post-payment recoupments. Every follow-up visit should show updated lab values, current medication details, and the patient’s clinical response to treatment, even briefly. A note like “LDL decreased from 185 to 140 mg/dL on current statin dose, continuing therapy” demonstrates active clinical management and protects the visit level billed.
Documentation Requirements That Make E78.5 Defensible
When E78.5 genuinely fits the encounter, the record still needs to include specific elements to survive payer review and audit scrutiny.
Provider statement in the assessment: The provider must document “hyperlipidemia,” “dyslipidemia,” or a similar clinical term explicitly in the assessment or problem list. A lab flag alone does not substitute for a provider statement.
Explanation of why the diagnosis remains unspecified: If the lipid panel is pending, note that fact directly. If the provider genuinely cannot specify the lipid type at this encounter, a brief clinical explanation in the note makes the E78.5 assignment defensible.
Lipid panel order or results: Even when results remain pending, showing that the provider ordered the appropriate diagnostic test demonstrates clinical diligence and supports the unspecified diagnosis.
Treatment plan: Document any dietary counseling, medication initiation, or lifestyle modification recommendations. Active management demonstrates medical necessity for the visit and the code.
Treating Hyperlipidemia: What the Clinical Record Should Reflect
Understanding how providers manage hyperlipidemia helps coders verify that the documentation matches the code and the E/M visit level billed. For patients carrying any E78 code, including E78.5 ICD 10, providers typically pursue:
Dietary modification as the first line of action. Reducing saturated fats, increasing soluble fiber, and cutting refined sugars all shift lipid panels in a positive direction. Documenting specific dietary counseling, even with a brief note, connects the clinical recommendation to the diagnosis code and strengthens the claim.
Statins for LDL management. When diet alone does not move numbers adequately, providers add statins such as atorvastatin or rosuvastatin to block the liver’s cholesterol production pathway. Once statin therapy starts, add Z79.899 to the claim to document long-term drug therapy.
Fibrates and omega-3s for triglyceride-dominant cases. When triglycerides drive the lipid problem, fibrates like fenofibrate target that specific pathway. Prescription-dose omega-3 fatty acids also lower triglycerides effectively. When the treatment plan targets triglycerides specifically, the documentation practically points the coder toward E78.1 rather than E78.5.
Routine lipid panel monitoring. Follow-up lipid panels four to twelve weeks after initiating or adjusting therapy show clinical response and generate new documentation that often supports upgrading from E78.5 to a more specific code on subsequent claims.
Frequently Asked Questions (FAQs)
Q1: What does the E78.5 ICD-10 code mean?
E78.5 is the ICD-10-CM code for “Hyperlipidemia, unspecified.” Providers and coders use this billable code when a patient carries elevated blood lipids but the provider’s documentation does not specify whether high cholesterol, high triglycerides, or both drive the problem. The 2026 edition took effect on October 1, 2025, and stays valid through September 30, 2026.
Q2: What is the difference between E78.5 vs E78.2?
E78.5 covers unspecified hyperlipidemia when the provider does not identify the exact lipid type. E78.2 covers mixed hyperlipidemia specifically, meaning both cholesterol and triglycerides run high simultaneously and the provider documents both elevations. When lab results and provider notes confirm both lipid types are elevated, E78.2 is the correct and more specific code. Using E78.5 in that scenario counts as under-coding.
Q3: When is it appropriate to use the E78.5 diagnosis code?
Use E78.5 when the provider documents hyperlipidemia without specifying the lipid type, when lab results are still pending at the time of coding, or when the transferred medical record references a history of lipid problems without identifying which type. Treat it as a temporary placeholder and update it once specific documentation becomes available.
Q4: Is the E78.5 ICD-10 code an acceptable ICD code for high cholesterol?
No. E78.5 covers unspecified hyperlipidemia, not high cholesterol specifically. When the provider documents elevated LDL cholesterol with normal triglycerides, the correct ICD code for high cholesterol is E78.00 for pure hypercholesterolemia, unspecified. Always choose E78.00 over E78.5 when documentation confirms that only cholesterol rises while triglycerides stay within normal ranges.
Q5: Can I use the dx code E78.5 for a routine screening visit?
No. E78.5 requires a confirmed or working diagnosis of hyperlipidemia. For a routine cholesterol screening in an asymptomatic patient with no confirmed lipid disorder, use Z13.220 for encounter for screening for lipoid disorders. Submitting E78.5 on a screening visit without a supporting confirmed diagnosis misrepresents the clinical scenario and invites payer denials.
Q6: What CPT codes commonly pair with E78.5 on claims?
CPT 80061, the lipid panel test, pairs with E78.5 when the provider orders diagnostic testing to evaluate the lipid disorder. For office visit management, CPT 99213 covers low-complexity encounters and CPT 99214 covers moderate-complexity visits. For dietary counseling, CPT codes 99401 through 99404 apply but require E78.5 or another E78 code as a supporting diagnosis to establish medical necessity.
Q7: Does using E78.5 frequently trigger audits?
Yes. Payers including Medicare and major commercial insurers track E78.5 usage rates across provider claims. Practices that submit E78.5 on nearly every lipid-related encounter raise red flags, especially when those same records contain lipid panel results that support more specific codes. Disproportionate use of unspecified codes signals documentation gaps and attracts focused audit attention.
Q8: Can E78.5 and E78.00 appear on the same claim?
No. These two codes overlap clinically. E78.00 covers pure hypercholesterolemia specifically, which already falls within the broader hyperlipidemia umbrella that E78.5 represents. Coding both creates a duplication error. When documentation supports E78.00, use that code alone. Reserve E78.5 only for situations where the provider genuinely does not specify the lipid type.
This article provides informational guidance on ICD-10-CM coding for educational purposes. Always apply current official ICD-10-CM guidelines and your organization’s compliance policies when making specific coding decisions.
Focus Keyword: E78.5 ICD 10 Slug: e78-5-icd-10-code-hyperlipidemia-unspecified Meta Title: E78.5 ICD-10 Code: Hyperlipidemia Unspecified Guide 2026 Meta Description: Learn the E78.5 ICD-10 code for hyperlipidemia, when to use it vs E78.2, coding rules, billing tips, and documentation requirements for 2026.