What Is Malaise ICD-10 Code ? Start Here Before You Code Anything
If you work in medical coding or billing, you have definitely come across Malaise ICD-10 Code on a claim. But here’s the thing — a lot of coders still use it wrong. That mistake costs practices thousands of dollars in denials every single year. So let’s break it all the way down, step by step.
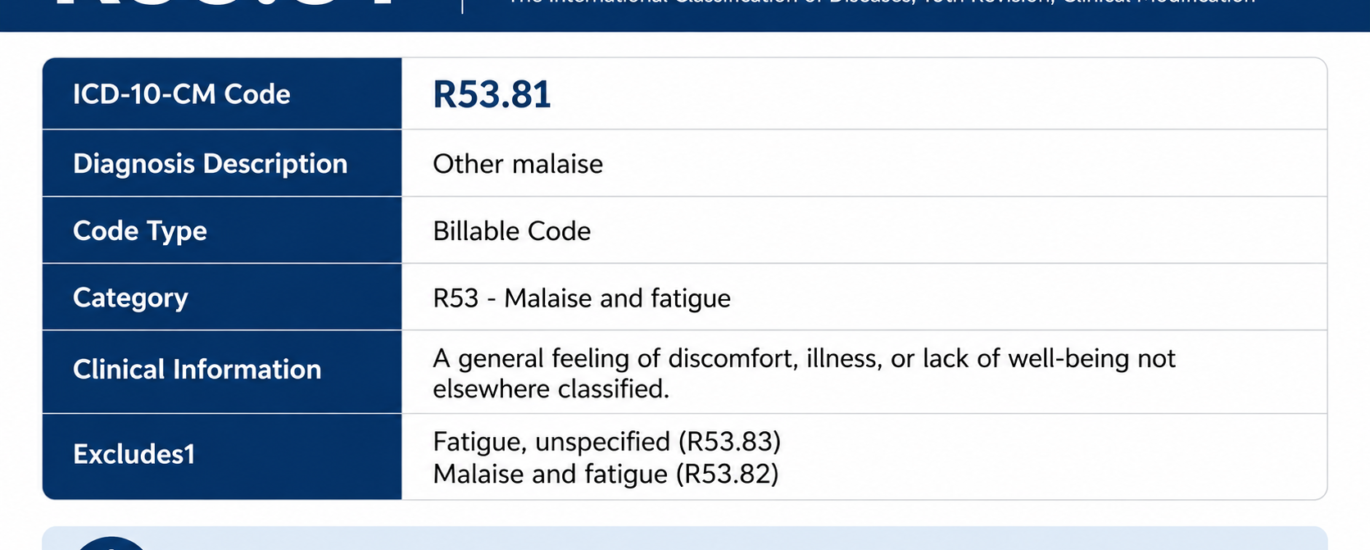
R53.81 is an ICD-10-CM diagnosis code that stands for “Other Malaise.” It falls under Chapter 18 of the ICD-10-CM classification system — Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified — specifically within the R50–R69 range covering general symptoms and signs.
In plain English, providers use this code when a patient walks in feeling genuinely terrible — tired, run-down, uncomfortable, just overall “off” — but no clear-cut underlying diagnosis exists yet. Think of it as the medical system’s way of saying, “Something is wrong, we are documenting it, and we are still figuring out what it is.”
Furthermore, the ICD 10 R53.81 code officially applies to adults between the ages of 15 and 124. As of the 2026 edition, it remains an active, specific, and billable code valid for HIPAA-covered transactions from October 1, 2025 through September 30, 2026.
2026 Meaning: What Does “Other Malaise” Actually Mean?
The word malaise comes from Old French, literally meaning “bad ease.” Honestly, that is a pretty spot-on description of what patients feel. Clinically speaking, malaise is a vague, non-specific symptom. It does not point to one particular organ or system. Instead, it describes that whole-body feeling of discomfort, physical unease, or general unwellness that patients often struggle to put into words.
How Doctors Define Malaise
Doctors generally describe malaise as:
- A general feeling of discomfort or unease without a clear cause
- A sense of being “out of sorts” or “not yourself”
- Chronic fatigue accompanied by physical symptoms that do not fit neatly into another category
Why the Word “Other” Matters in R53.81
The key word in the Malaise ICD-10 Code is “Other.” Specifically, this means providers use this code for malaise cases that do not fall under the more defined subcategories of R53 — like neoplastic-related fatigue (R53.0), generalized weakness (R53.1), or chronic fatigue syndrome (R53.82). In other words, if the patient’s condition fits a more specific category, you go there first. Consequently, R53.81 becomes the fallback for everything that does not fit elsewhere.
Symptoms Commonly Linked to R53.81
Since other malaise is a symptom code rather than a definitive disease, the clinical presentation varies widely from patient to patient. That is actually what makes it tricky to document correctly. Here are the most common symptoms that providers typically associate with an R53.81 diagnosis:
- Persistent general fatigue that does not improve with rest
- Vague physical discomfort with no identifiable site-specific pain
- Low energy levels that interfere with daily activity
- Feeling physically weak or run-down without objective muscle weakness
- Mild cognitive fog or difficulty concentrating
- Sleep disturbances, including both insomnia and hypersomnia
- Low mood or emotional flat affect connected to the physical discomfort
- Lack of motivation or drive, not tied to a psychiatric diagnosis
- Decreased appetite or general changes in eating patterns
Why Symptom Documentation Matters So Much
Now, here is something critical for coders to remember: these symptoms are largely subjective. Patients report them differently. One person calls it “bone-tired exhaustion,” while another says they just feel “blah” all the time. Therefore, your documentation must capture the specific language the provider used — because that language supports the Malaise ICD-10 Code and keeps your claim clean during an audit.
Common Causes of Other Malaise
Because R53.81 is a symptom code, the causes cover essentially anything that makes a person feel generally unwell. However, healthcare providers typically explore the following root causes before they land on this code:
Infectious or Post-Infectious Triggers
Viral infections — think influenza, COVID-19 sequelae, or mononucleosis — rank among the top drivers of malaise. Moreover, patients recovering from illness often experience lingering general unwellness even after the infection itself resolves. In those cases, Malaise ICD-10 Code works as a valid temporary placeholder while further workup continues.
Chronic Medical Conditions
Additionally, underlying chronic conditions frequently produce malaise as a secondary symptom. These include:
- Diabetes mellitus
- Hypothyroidism
- Anemia
- Autoimmune disorders such as lupus and rheumatoid arthritis
- Chronic kidney disease
- Heart failure
When providers confirm one of these conditions, coders should assign the specific disease code and move R53.81 to a secondary role — or drop it entirely if it adds no clinical value.
Psychological and Behavioral Factors
Depression, anxiety, and chronic stress strongly connect to physical malaise. The mind-body link is real. In 2026, clinicians increasingly document these intersections. However, once a provider confirms a mental health diagnosis, coders should assign that diagnosis directly rather than defaulting to R53.81.
Nutritional Deficiencies
Similarly, iron deficiency, vitamin D deficiency, B12 deficiency, and related nutritional issues frequently cause patients to feel persistently unwell. As a result, lab workup usually forms part of the diagnostic path for these presentations.
Medication Side Effects
Certain drug classes — particularly chemotherapy agents, antihypertensives, and antidepressants — list general malaise as a documented side effect. In those cases, an adverse effect code from the T36–T50 range may also apply alongside R53.81.
Idiopathic Cases
Sometimes, after a thorough workup, providers find no identifiable cause. That is precisely when ICD 10 R53.81 works as the primary working diagnosis. The provider documents that a full evaluation occurred, other causes were ruled out, and the patient’s condition gets coded as other malaise.
Billing Tips for Malaise ICD-10 Code in 2026
This is where the rubber meets the road. Billing with R53.81 incorrectly is one of the fastest ways to trigger a claim denial or, worse, a compliance audit. Here is what you absolutely need to know heading into 2026:
Tip 1: R53.81 Is Billable — But Only With Strong Documentation
Yes, the R53.81 diagnosis code is a specific, billable code. However, “billable” does not mean “bill it and forget it.” You need clinical documentation that supports the code. At a minimum, the record must include:
- Duration and onset of the malaise
- Impact on the patient’s daily functioning
- Results of any diagnostic workup the provider performed
- Clinical decision-making around ruling out other diagnoses
Tip 2: Do Not Use It as a Principal Diagnosis When a Definitive Dx Exists
This is one of the biggest rules in ICD-10-CM guidelines. Specifically, do not assign R53.81 as the principal diagnosis when a related definitive diagnosis already exists. For example, if a patient has confirmed hypothyroidism causing their malaise, code the hypothyroidism — not R53.81.
Tip 3: Know Your CPT Pairings
When billing R53.81, the most commonly paired CPT codes include:
| CPT Code | Description |
|---|---|
| 99202–99215 | Office/outpatient E&M services (new/established patients) |
| 99381–99397 | Preventive medicine evaluations |
| 99401–99404 | Preventive medicine counseling |
| 96150–96155 | Health and behavior assessment/intervention |
Tip 4: R53.81 Applies to Adults Only
The code carries an Adult Dx restriction (ages 15–124). Therefore, applying it to pediatric patients is a coding error that will immediately trigger a denial. For pediatric malaise presentations, always check the appropriate codes under the symptom categories.
Tip 5: Watch Your Type 1 Excludes
The ICD-10-CM Type 1 Excludes note on R53.81 means certain codes cannot appear on the same claim. For instance, do not pair R53.81 with R54 (age-related physical debility) on the same submission. That combination violates a hard exclusion rule.
Related ICD-10 Codes You Need to Know
Understanding where Malaise ICD-10 Code sits in the broader R53 family — and how it relates to nearby codes — is critical for accurate, compliant coding.
| ICD-10 Code | Description |
|---|---|
| R53.81 | Other malaise |
| R53.0 | Neoplastic (malignant) related fatigue |
| R53.1 | Weakness (generalized) |
| R53.2 | Functional quadriplegia |
| R53.82 | Chronic fatigue, unspecified |
| R53.83 | Other fatigue |
| R54 | Age-related physical debility |
| R41.3 | Other amnesia |
Additionally, when documenting malaise that ties to specific underlying conditions, coders often pair R53.81 with:
- D50.9 — Iron deficiency anemia, unspecified
- E11.9 — Type 2 diabetes mellitus without complications
- F32.9 — Major depressive disorder, single episode, unspecified
- E03.9 — Hypothyroidism, unspecified
The right combination of codes tells the full clinical story. Furthermore, that complete story is what gets your claim paid on the first submission.
2026 Common Mistakes Coders Make with R53.81
Let’s talk real talk here. These are the most frequent coding errors that keep showing up in 2026 audits — and every single one of them is completely preventable.
Mistake #1: Using R53.81 as a Catch-All Code
R53.81 is not a dumping ground for any patient who seems tired or unwell. For instance, submitting it without proper workup documentation — or as a lazy substitute for a more specific code — puts your practice at serious compliance risk. Moreover, payers grow smarter every year. AI-driven claim reviews now flag symptom-only codes more aggressively than ever in 2026.
Mistake #2: Coding R53.81 Alongside R54 Simultaneously
This directly violates the Type 1 Excludes rule. R53.81 and R54 cannot coexist on the same claim. Therefore, choose the one that best fits the clinical picture and move on.
Mistake #3: Submitting R53.81 as the Primary Code When a Definitive Diagnosis Exists
If the provider already documented a confirmed underlying cause — say, anemia or hypothyroidism — that condition becomes the primary code. As a result, R53.81 steps down to secondary, or gets dropped entirely if it does not add clinically meaningful information.
Mistake #4: Vague or Missing Onset Documentation
“Patient feels tired” is simply not enough. In 2026, Medicare and private payers specifically flag claims with vague symptom descriptions and no timeline. You need documented onset dates, duration, and functional impact on the patient’s daily life.
Mistake #5: Applying R53.81 to Pediatric Patients
The code carries an Adult Dx restriction. Consequently, using it for patients under 15 is an automatic error that triggers denials. Always verify the age restriction before assigning this code.
Mistake #6: Confusing R53.81 with R53.82 or R53.83
These three codes look similar, but they mean very different things:
- R53.81 = Other malaise (non-specific general unwellness)
- R53.82 = Chronic fatigue, unspecified (lasting 6+ months)
- R53.83 = Other fatigue (different presentation)
Using them interchangeably is incorrect. Additionally, it distorts diagnostic data at a population level, which matters more than ever as CMS increases data quality monitoring in 2026.
2026 Updates: What Is New for R53.81 This Year
Heading into fiscal year 2026, which officially began October 1, 2025, several important updates and trends directly impact how you handle R53.81 claims.
ICD-10-CM 2026 Official Effective Date
First and foremost, the 2026 edition of ICD-10-CM R53.81 became effective on October 1, 2025, and remains valid through September 30, 2026. This reflects the American ICD-10-CM version — international ICD-10 versions may differ.
Increased Payer Scrutiny on Symptom-Only Codes
In 2025, Medicare Advantage rejections rose sharply for symptom-based codes without robust documentation. That trend continues hard into 2026. Payers — including private insurers and CMS — now increasingly require diagnostic clarification when codes like R53.81 appear repeatedly on the same patient account without an evolving diagnostic workup.
AI-Driven Claim Reviews Are Now Standard
Furthermore, many major payers now run AI-assisted pre-payment claim review systems. These systems specifically target patterns like symptom codes as standalone principal diagnoses, missing onset documentation, and repeated use of non-specific codes without progress toward a definitive diagnosis. As a result, your documentation quality directly determines your payment speed.
Greater Emphasis on Social Determinants of Health (SDOH)
In 2026, CMS guidelines push harder for SDOH codes to accompany symptom-based diagnoses like R53.81. Specifically, if a patient’s malaise connects to food insecurity, housing instability, or work-related stress, adding the appropriate Z-code alongside R53.81 strengthens your documentation considerably and builds a fuller clinical picture.
MS-DRG V43.0 Updates
Finally, under MS-DRG V43.0 — applicable October 1, 2025 through September 30, 2026 — R53.81 maps to specific diagnostic related groups. Knowing which DRG applies helps facilities optimize reimbursement while staying fully within compliance guardrails.
How to Diagnose and Document Malaise Correctly
Diagnosing other malaise properly follows a structured, logical path. Since it is a symptom rather than a standalone disease, the documentation must show the provider’s full clinical reasoning — not just the patient’s complaint.
Step 1: Capture the Full Patient History
First, document the onset, duration, timing, and any aggravating or relieving factors the patient describes. The more specific this history is, the stronger your claim becomes.
Step 2: Record Physical Examination Findings
Even when findings appear largely normal, document exactly what the provider assessed. Normal findings, when properly recorded, actually support the use of R53.81 by showing the provider actively ruled out other conditions.
Step 3: Order and Document Diagnostic Workup
Next, the provider should order clinically appropriate labs — typically a CBC, comprehensive metabolic panel, thyroid function tests, vitamin levels, and infection panels. Document every test ordered and every result received.
Step 4: Screen for Mental Health Factors
Additionally, if psychological contributors seem possible, document a mental health screening using a validated tool like the PHQ-9 or GAD-7. This step matters especially in 2026, given the growing overlap between behavioral health documentation and medical billing.
Step 5: Establish the Differential Diagnosis
Before assigning R53.81, the provider must document the differential diagnosis. In other words, the record should clearly show what other conditions the provider considered and why they ruled them out.
Step 6: Assign R53.81 Only After the Above Steps
Finally, assign the R53.81 diagnosis code only after the provider has appropriately considered and ruled out other specific conditions — or while workup remains pending. This documentation trail protects your claim and proves medical necessity. Without it, R53.81 is just a three-digit guess on a piece of paper — and payers absolutely know that.
Frequently Asked Questions (FAQ)
Q: Is R53.81 a billable ICD-10 code in 2026? Yes, absolutely. R53.81 is a specific, billable ICD-10-CM code valid from October 1, 2025 through September 30, 2026. Furthermore, providers can use it for reimbursement when clinical documentation properly supports it.
Q: What is the difference between R53.81 and R53.82? R53.81 covers “other malaise” — a general, non-specific sense of unwellness. R53.82, on the other hand, specifically refers to “chronic fatigue, unspecified,” meaning fatigue lasting six months or more. Therefore, they are distinct codes and providers should never use them interchangeably.
Q: Can R53.81 serve as a principal diagnosis? Yes, but only when no definitive underlying diagnosis exists yet. ICD-10-CM guidelines specifically state that providers should NOT use R53.81 as the principal diagnosis when a related confirmed diagnosis already appears in the record.
Q: Can R53.81 and R53.1 appear together on a claim? Yes, in some cases these two codes can coexist — specifically when both other malaise and generalized weakness appear separately documented and carry independent clinical significance. However, make sure documentation clearly supports both.
Q: What age group does R53.81 apply to? R53.81 carries an Adult Dx designation, covering patients aged 15 to 124. Consequently, coders should not apply it to pediatric patients under 15.
Q: What CPT codes pair most often with R53.81? The most common pairings include E&M codes 99202–99215 for office visits, and additionally 96150–96155 for health and behavior assessment when behavioral health factors contribute to the clinical picture.
Q: How do I avoid claim denials when using R53.81? Above all, document clearly. Include the onset date, duration, functional impact, workup results, and the provider’s clinical decision-making process. Never submit R53.81 as a standalone code without supporting documentation.
Q: Does R53.81 apply to COVID-19 long-haul symptoms? Yes, in certain situations. Providers can use it when a patient presents with lingering general malaise after a COVID-19 infection and no more specific post-COVID code applies. However, always check for U09.9 (Post-COVID-19 condition) before defaulting to R53.81.
Final Takeaway: Use R53.81 the Right Way in 2026
Here is the bottom line: R53.81 is a legitimate, powerful, and frequently needed code in the ICD-10-CM toolkit. It gives providers and coders a precise way to capture and bill for a real clinical presentation — general malaise — that genuinely impacts patients and drives healthcare utilization every single day.
But it only works when you use it correctly. Strong documentation, proper code sequencing, age-appropriate application, and solid awareness of excluded codes all make the difference between clean claims and costly denials.
In 2026, with payer scrutiny at an all-time high and AI-driven pre-payment reviews now standard across major insurers, there is simply no room for sloppy symptom coding. The R53.81 diagnosis code is your friend — as long as you treat it with the clinical precision it deserves.
Stay current. Code smart. And when in doubt, always document more.
Article written by a 10+ year experienced medical content strategist specializing in ICD-10-CM coding, clinical billing compliance, and healthcare revenue cycle management.