

If you have ever stared at a lab report and wondered what does high PSA mean, you are definitely not alone. Thousands of men get this exact question every single day, and just as many medical coders sit at their desks trying to nail down the right diagnosis code for the claim. That is where R97.20 comes into the picture. It is the ICD-10-CM code tied to elevated PSA levels, and it shows up constantly in urology offices, primary care clinics, and billing departments across the country.
This guide walks through everything tied to R97.20 in plain, simple language. We will cover the meaning, the symptoms that often accompany a high reading, the causes behind it, billing tips that actually save you from denied claims, related codes you need to know, common mistakes coders make, and the 2026 updates that changed how this code gets used. By the end, you will have a clear, practical understanding of this code whether you are a patient trying to make sense of a lab slip or a coder trying to avoid a rejected claim.
What Does R97.20 Mean
R97.20 is the ICD-10-CM diagnosis code for elevated prostate specific antigen, commonly shortened to PSA. This code falls under chapter eighteen of the ICD-10 system, which covers symptoms, signs, and abnormal clinical findings that do not have a confirmed diagnosis attached yet. In simpler terms, R97.20 tells the payer and the medical record that a man’s PSA blood test came back higher than the normal PSA range for men, but no cancer diagnosis has been confirmed.
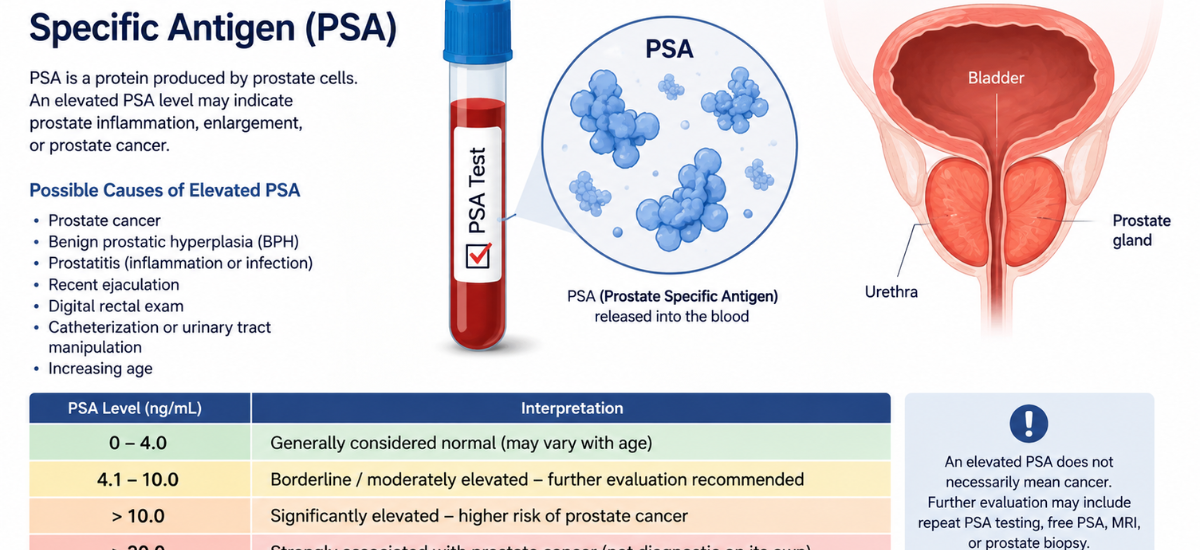
This distinction matters a lot. R97.20 is not a cancer code. It is a marker that says something is off and needs more investigation. Doctors lean on this code constantly because PSA elevation does not automatically mean prostate cancer. It just means the number on the lab report sits above the typical reference threshold, which is usually around 4.0 ng/mL, though that threshold can shift slightly depending on age and lab standards.
Because R97.20 only applies to abnormal findings, it gets paired frequently with follow-up testing, repeat labs, or imaging while the care team figures out the underlying cause.
Symptoms Linked to Elevated PSA
Here is something that surprises a lot of patients: elevated PSA itself does not cause symptoms. PSA is just a protein that shows up in blood work. However, the conditions that drive PSA upward often come with their own signs. Recognizing these symptoms helps both patients and providers connect the dots faster.
Common symptoms that often accompany a high PSA reading include:
- Frequent urination, especially at night
- Weak or interrupted urine flow
- A feeling that the bladder never fully empties
- Pain or burning during urination
- Pelvic discomfort or lower back pain
- Blood in urine or semen in rarer cases
If a patient walks in with these symptoms and the PSA test results explained later show an elevated number, the provider typically moves toward additional diagnostic steps rather than jumping straight to a cancer workup. That is exactly why context matters so much when coding R97.20.
Causes of Elevated PSA Levels
There is a long list of reasons a PSA level might creep upward, and most of them have nothing to do with cancer. Below is a breakdown of the most frequent elevated PSA levels causes seen in clinical practice today.
| Cause | How It Affects PSA |
|---|---|
| Benign prostatic hyperplasia (BPH) | Enlarged prostate tissue produces more PSA naturally |
| Prostatitis (infection or inflammation) | Inflammation pushes PSA levels up temporarily |
| Recent ejaculation | Can cause a short-term spike in PSA |
| Urinary tract infection | Irritates prostate tissue and raises PSA |
| Recent prostate biopsy or procedure | Physical trauma to the gland increases PSA |
| Vigorous exercise, including cycling | Pressure on the prostate area can elevate readings |
| Certain medications or supplements | Some substances interfere with normal PSA regulation |
| Prostate cancer | A confirmed possibility, but only one of many causes |
This is exactly why so many men search high PSA but no cancer after getting their results back. The reality is that a single elevated reading is rarely conclusive on its own. Doctors usually repeat the test, review the PSA levels by age chart for context, and consider the patient’s full history before deciding on next steps.
Age plays a noticeable role too. PSA naturally rises a bit as men get older simply because the prostate grows larger over time. A PSA of 3.5 ng/mL might be considered borderline in a 50 year old but fairly unremarkable in someone closer to 70.
Billing Tips for R97.20
Getting the billing side right matters just as much as understanding the clinical picture. Insurance companies scrutinize PSA-related claims closely, so a little extra care during documentation goes a long way toward avoiding denials.
Document the Exact PSA Value
Always make sure the actual number from the lab report appears in the chart note. Vague language like “PSA elevated” without a number is one of the fastest ways to trigger a request for additional records or an outright denial.
Pair With the Correct CPT Code
R97.20 is typically billed alongside CPT 84153 for total PSA testing or CPT 84154 when a free PSA test follows an indeterminate result. Matching the diagnosis code with the correct procedure code keeps the claim clean and reduces back-and-forth with the payer.
Separate Screening From Diagnostic Visits
If a patient comes in purely for a routine screening with no symptoms, the encounter should lean on Z12.5 first, not R97.20. R97.20 only becomes appropriate once the test result actually comes back abnormal. Mixing these up is one of the most frequent reasons claims bounce back.
Avoid Using R97.20 After a Cancer Diagnosis Is Confirmed
Once a patient has a confirmed diagnosis of prostate cancer, the coding shifts. C61 becomes the primary code for active disease, and R97.21 takes over for rising PSA after treatment. Continuing to use R97.20 after a cancer diagnosis is established creates a mismatch that auditors flag quickly.
Support Medical Necessity With Clinical Context
Payers want to see why the test was ordered. A short note explaining symptoms, prior abnormal results, or a family history of prostate issues strengthens the medical necessity argument and speeds up reimbursement.
Related Codes You Should Know
Coders working with R97.20 regularly bump into several closely related codes. Knowing how these connect helps prevent mix-ups during chart review.
- R97.21 – Rising PSA following treatment for malignant neoplasm of the prostate, used specifically for patients with a prior cancer history
- C61 – Malignant neoplasm of the prostate, used once cancer is confirmed
- N40.0 – Benign prostatic hyperplasia without lower urinary tract symptoms, often paired when BPH is the likely driver
- N40.1 – Benign prostatic hyperplasia with lower urinary tract symptoms
- Z12.5 – Encounter for screening for malignant neoplasm of the prostate, used for asymptomatic routine screening visits
- Z85.46 – Personal history of malignant neoplasm of the prostate, useful for monitoring patients post-treatment
- N41.0 – Acute prostatitis, relevant when infection is the suspected cause of elevated PSA
Keeping this list handy speeds up daily coding work and reduces the chance of choosing a code that does not match the clinical story.
Common Mistakes Coders Make With R97.20
Even seasoned coders slip up occasionally, and these mistakes tend to repeat across practices nationwide.
- Using R97.20 for screening visits. Screening encounters belong under Z12.5 first, not R97.20.
- Skipping the actual PSA number in documentation. Auditors want the value, not just the word “elevated.”
- Failing to update the code after a cancer diagnosis. Once cancer is confirmed, R97.20 should step aside for C61 or R97.21.
- Overlooking BPH or prostatitis as contributing factors. Adding N40.0 or N41.0 when appropriate paints a fuller clinical picture.
- Not linking the diagnosis to the correct CPT code. Mismatched CPT and ICD-10 pairings are a leading cause of claim rejections.
- Assuming a single elevated reading confirms a chronic issue. Many providers order a repeat test before committing to further workup, and documentation should reflect that plan.
Avoiding these missteps keeps claims moving smoothly and protects practices during compliance reviews.
2026 Updates Affecting R97.20
The fiscal year 2026 ICD-10-CM code set, which became effective on October 1, 2025, brought one of the larger refreshes in recent memory, with several hundred new codes added system-wide along with dozens of revisions across multiple chapters. While R97.20 itself was not deleted or restructured, it remains active and billable under the current code set, valid through September 30, 2026.
What changed broadly across the 2026 update is the push toward greater specificity in documentation. Coding leaders have emphasized that clinical notes now need to support more detailed context, which directly affects how R97.20 gets used day to day. Practices that lean on vague PSA documentation will likely see more denials in 2026 simply because payers are tightening expectations around specificity across the board.
Another trend worth watching is the growing use of the free to total PSA ratio test, billed under CPT 84154, as a reflex step when an initial PSA lands in that gray zone between four and ten. This approach helps providers stratify cancer risk without rushing into more invasive procedures, and R97.20 still applies as the diagnosis code supporting that reflex testing.
Telehealth-driven follow-up visits for abnormal lab results have also grown steadily, meaning more PSA discussions happen virtually before an in-person visit gets scheduled. Coders should expect telehealth modifiers to show up more frequently alongside R97.20 going into the rest of 2026.
Frequently Asked Questions
What is the ICD-10 code for elevated PSA? The code is R97.20. It applies to elevated prostate specific antigen findings without a confirmed prostate cancer diagnosis.
Does R97.20 mean someone has prostate cancer? No. R97.20 simply documents an abnormal lab finding. Plenty of conditions besides cancer cause PSA to rise, including BPH, prostatitis, and recent physical activity.
What is considered a normal PSA range for men? Most labs treat anything under 4.0 ng/mL as within normal limits, though the acceptable range can shift slightly based on age and individual lab standards.
Can R97.20 be used for a screening visit? Generally no. Screening visits without symptoms typically use Z12.5. R97.20 becomes appropriate once an actual abnormal result comes back.
What code replaces R97.20 once cancer is confirmed? C61 becomes the primary code for active prostate cancer. R97.21 applies specifically when PSA rises again after prior cancer treatment.
Why did my PSA come back high if I do not have cancer? High PSA but no cancer is actually a common outcome. Causes range from an enlarged prostate to a recent infection, vigorous exercise, or even recent ejaculation before the test.
How often should PSA be retested after an elevated result? Many providers repeat the test within four to twelve weeks to rule out a temporary spike before pursuing further workup, though the exact timing depends on the individual case and provider judgment.
Final Thoughts
R97.20 plays a small but mighty role in both clinical documentation and medical billing. For patients, understanding this code can ease a lot of unnecessary worry after seeing an unexpected lab result. For coders and billing teams, getting the documentation, CPT pairing, and follow-up coding right protects revenue and keeps compliance teams happy. As the 2026 ICD-10-CM landscape continues pushing for sharper specificity, staying current on how R97.20 fits into the bigger picture will only become more valuable for everyone involved in prostate health care.




