What Are CPT Codes: Understanding the Fundamentals
Current Procedural Terminology, commonly referred to as CPT codes, forms the backbone of medical billing and healthcare reimbursement across the United States. Essentially, these five-digit numerical codes serve as the universal language that healthcare providers use to communicate with insurance payers about what services and procedures they’ve delivered to patients.
The Bridge Between Clinical Care and Billing
Think of CPT codes as the critical bridge between clinical care and financial reimbursement. When a doctor performs a colonoscopy, runs lab tests, or provides physical therapy, medical coders must translate these clinical actions into specific CPT codes. Subsequently, insurance companies use these codes to determine payment amounts, coverage eligibility, and claim processing.
Annual Updates Reflect Healthcare Evolution
Notably, the American Medical Association maintains and updates the CPT code set annually. Every January 1st, new codes take effect, old codes get retired, and existing codes receive updates. This continuous evolution reflects the changing landscape of healthcare delivery, technological advancement, and clinical innovation. Therefore, understanding these codes isn’t just important for billing accuracy; it directly impacts patient care, practice revenue, and compliance with healthcare regulations.
The 2026 CPT Code Update: What Changed and Why It Matters
The Scale of Change
Notably, the 2026 CPT update brings substantial changes that medical coders must grasp to avoid claim denials and compliance issues. Specifically, the American Medical Association introduced 288 brand new codes, removed 84 outdated codes, and revised 46 existing ones, resulting in 418 total editorial changes. Consequently, this represents one of the most significant annual updates in recent memory.
Why These Changes Matter
These changes didn’t happen randomly. Rather, they reflect real shifts in how healthcare gets delivered. For instance, remote patient monitoring continues expanding. Simultaneously, artificial intelligence now plays a role in clinical diagnostics. Additionally, minimally invasive procedures keep evolving, and complex surgical techniques emerge regularly. Therefore, the CPT code set must keep pace with this innovation.
Compliance Implications for Coders
For medical coders working in 2026, staying current with these changes moves beyond professional development. Indeed, it becomes a compliance necessity. Specifically, using outdated codes can trigger claim denials, payment delays, and regulatory issues. More importantly, incorrect coding can prevent patients from getting the services they need covered by insurance.
Breaking Down Key CPT Code Categories
Category I Codes: The Standard
Importantly, Category I codes represent the most commonly used codes in medical billing. Specifically, these five-digit codes describe established medical procedures and services that have solid clinical data supporting their use. For instance, when you think of CPT codes, you’re typically thinking of Category I codes like 45378 for diagnostic colonoscopy or 97161 for physical therapy evaluation.
Category II Codes: Tracking and Performance
Additionally, Category II codes follow a different pattern with four digits plus the letter F. Importantly, these optional codes help track quality measures and performance metrics. As an illustration, code 3008F reports Body Mass Index documentation during routine checkups. Significantly, while these codes don’t get billed to insurance, they provide valuable data for practice performance analysis and clinical outcome tracking.
Category III Codes: Emerging Procedures
Furthermore, Category III codes, formatted as four digits followed by T, describe emerging medical services, procedures, and technologies that don’t yet have enough data for Category I status. Essentially, these temporary codes allow the healthcare system to track new treatments while evidence accumulates. As a result, many 2026 additions fall into this category, particularly codes for AI-assisted diagnostics and advanced imaging techniques.
CPT Code for Colonoscopy: Essential Procedures and Distinctions
Ultimately, colonoscopy coding requires precision because the same procedure can warrant different codes depending on whether it’s screening or diagnostic and what interventions occur during the procedure.
Screening Colonoscopy Codes
Specifically, for Medicare patients undergoing screening colonoscopies, coders must use G-codes rather than standard CPT codes:
- G0105: Colorectal cancer screening for individuals at high risk (includes family history of colon cancer, prior polyps, or risk factors)
- G0121: Colorectal cancer screening for individuals not meeting high-risk criteria
Why G-Codes Matter for Medicare
Importantly, using G0105 or G0121 ensures Medicare patients receive preventive benefits without unnecessary out-of-pocket costs. This distinction matters significantly. Furthermore, submitting 45378 instead of the appropriate G-code triggers automatic claim denials on Medicare claims.
Commercial Insurance Screening Rules
Conversely, for commercial insurance patients, screening colonoscopies get billed using CPT code 45378 with modifier 33. Notably, the 33 modifier signals that the primary purpose involved delivering evidence-based preventive services, ensuring proper coverage under the Affordable Care Act.
Diagnostic Colonoscopy Codes
Conversely, when a colonoscopy gets performed for diagnostic indications (patient has symptoms or abnormal findings), different codes apply entirely:
- 45378: Diagnostic colonoscopy with or without specimen collection (this represents the “base code”)
- 45379: Colonoscopy with removal of foreign body
- 45380: Colonoscopy with biopsy, single or multiple
- 45381: Colonoscopy with directed submucosal injection for tattooing or hemostasis
- 45382: Colonoscopy with control of bleeding using any method
- 45384: Colonoscopy with removal of tumor, polyp, or lesion using hot biopsy forceps
- 45385: Colonoscopy with removal of tumor, polyp, or lesion using snare technique
- 45386: Colonoscopy with dilation using balloon or bougie
- 45388: Colonoscopy with ablation of tumor, polyp, or lesion
- 45389: Colonoscopy with endoscopic stent placement
- 45390: Colonoscopy with endoscopic mucosal resection
- 45391: Colonoscopy with endoscopic ultrasound exam
- 45392: Colonoscopy with endoscopic ultrasound-guided needle aspiration or biopsy
- 45397: Colonoscopy with transendoscopic stent placement
Understanding the Code Hierarchy
Additionally, these codes follow a hierarchical structure. Notably, code 45378 serves as the foundational diagnostic code. Subsequently, all therapeutic codes (45379-45398) represent additional interventions performed during the same session. Therefore, proper code selection depends entirely on documenting the highest-level intervention performed.
The Screening-to-Diagnostic Conversion Challenge
Significantly, one of the trickiest aspects of colonoscopy coding involves screening procedures that convert to diagnostic during the examination. Essentially, when a colonoscopy starts as routine screening but polyps are discovered and removed, the coding changes dramatically.
Medicare Conversion Rules
Specifically, for Medicare patients, attach modifier PT (colorectal cancer screening test converted to diagnostic test or other procedure) to the appropriate therapeutic code. For example, if a Medicare patient undergoes G0121 screening and a polyp gets removed via snare technique, bill 45385-PT.
Important Coinsurance Changes for 2026
Notably, as of 2026, Medicare patients remain responsible for 15% coinsurance when a screening colonoscopy converts to therapeutic services. Moreover, this percentage drops to 10% from 2027 through 2029, and reaches 100% coverage by 2030. Therefore, patients should understand this change when planning their procedures.
Commercial Insurance Conversion Guidelines
Conversely, for commercial insurance patients, if documentation clearly states the procedure began as screening, submit the therapeutic code with modifier 33 to ensure preventive benefits apply. This distinction proves critical in preventing unexpected patient bills.
Common Colonoscopy Coding Mistakes
Medical coders frequently stumble on these colonoscopy errors that trigger denials and compliance issues.
Mistake 1: Using Base Code with Therapeutic Codes
Notably, one common error involves submitting the diagnostic base code alongside therapeutic codes like snare polypectomy. Specifically, insurance systems flag this combination as bundled services and automatically deny payment. Additionally, this mistake often results in patient billing issues and practice revenue loss.
Mistake 2: Forgetting Modifiers on Medicare Conversions
Furthermore, another frequent mistake occurs when coders omit modifier PT when screening converts to therapeutic. Consequently, this omission results in patients facing unexpected bills. Therefore, always verify that Medicare conversion claims include proper modifier coding.
Mistake 3: Incomplete Documentation of Procedures
Moreover, failing to specify polyp location, removal technique, or number of polyps discovered creates compliance vulnerabilities. Importantly, this type of incomplete documentation leads to audits and claim issues. Thus, detailed operative notes prove essential for clean claims.
Mistake 4: Using Wrong Screening Codes for Medicare
Finally, billing 45378 for Medicare patients instead of G0105 or G0121 triggers automatic denials. Consequently, this basic coding error ranks among the most preventable denial reasons. Therefore, always verify patient insurance before code selection.
CPT Code for Physical Therapy: Evaluation and Treatment
Physical therapy billing centers on evaluation codes plus treatment procedure codes. The evaluation codes determine the initial visit’s complexity, while treatment codes describe the interventions provided.
Physical Therapy Evaluation Codes
The current evaluation structure uses three tiered complexity levels:
97161: Low Complexity Physical Therapy Evaluation
- Requires: No personal factors and/or comorbidities OR 1-2 personal factors
- Examination: Addresses 1-2 body system elements
- Presentation: Stable conditions
- Typical time: Approximately 20 minutes face-to-face
- Appropriate for: Simple ankle sprains, minor neck strain, basic mobility issues
97162: Moderate Complexity Physical Therapy Evaluation
- Requires: 3 or more personal factors and/or comorbidities
- Examination: Addresses 3 or more body system elements total
- Presentation: Worsening or improving conditions
- Typical time: Approximately 30 minutes face-to-face
- Appropriate for: Multiple joint involvement, some medical comorbidities, evolving conditions
97163: High Complexity Physical Therapy Evaluation
- Requires: 3 or more personal factors and/or comorbidities
- Examination: Addresses 4 or more body system elements total
- Presentation: Unstable conditions with significant medical complexity
- Typical time: Approximately 45 minutes face-to-face
- Appropriate for: Multiple diagnoses, significant medical history, complex functional limitations
97164: Physical Therapy Re-evaluation Used when significant changes in patient condition or functional status warrant plan of care revision. Unlike evaluation codes, re-evaluation gets used when established patients show meaningful improvement or deterioration requiring new assessment.
Critical Complexity Selection Errors
Significantly, many physical therapy practices underbill by routinely using 97162 (moderate) for all evaluations. In fact, this “safe middle ground” approach leaves money on the table. Moreover, proper evaluation of each patient’s history, examination complexity, and clinical decision-making requirements ensures appropriate reimbursement.
Conversely, some facilities engage in overcoding by selecting 97163 when documentation only supports 97162. Furthermore, payer audits quickly identify these patterns, leading to payment recoupments and serious compliance concerns. Therefore, accurate complexity assessment proves essential for both billing integrity and practice sustainability.
Treatment Procedure Codes
Additionally, beyond evaluation codes, physical therapists bill treatment codes based on the interventions provided:
- 97110: Therapeutic exercises for strength, endurance, flexibility, and range of motion
- 97112: Neuromuscular re-education for balance, coordination, and proprioception
- 97140: Manual therapy including mobilization, manipulation, and manual traction (discussed further for pregnancy massage applications)
- 97162-97163: These modalities continue describing treatment when therapists blend multiple techniques
- 97530: Therapeutic activities and exercises tailored to meet functional goals
- 97150: Group physical therapy
The 8-Minute Rule Explained
Importantly, physical therapy billing uses the “8-Minute Rule,” meaning coders bill one unit for every 8 minutes spent on timed services. Notably, accumulating minutes across multiple 15-minute unit codes requires careful documentation and calculation. Therefore, understanding this rule prevents both underbilling and compliance audits.
CPT Code for Pregnancy Massage: Medical Necessity and Billing
Pregnancy massage billing presents unique challenges because insurance companies scrutinize massage therapy codes heavily, requiring clear demonstration of medical necessity.
Understanding Pregnancy Massage CPT Codes
97124: Therapeutic Massage Therapy
- Description: Massage technique including effleurage, petrissage, and tapotement
- Application: Pregnancy-related muscle tension, circulation improvement
- Time-based: Billed in 15-minute increments
- Insurance perspective: Viewed as comfort-based unless documented medical necessity exists
- Coverage: Highly variable among payers; many require pre-authorization
97140: Manual Therapy Procedures
- Description: Manual techniques including myofascial release, joint mobilization, and manual traction
- Application: Pregnancy-related sciatica, sacroiliac joint dysfunction, lymphatic drainage
- Time-based: Billed in 15-minute increments
- Insurance perspective: Viewed as more clinical when properly documented
- Coverage: More frequently covered when provided by licensed PT/OT with physician referral
97530: Therapeutic Activities
- Description: Exercises and activities designed to foster goal attainment
- Application: Guided movements for pregnancy comfort, labor preparation exercises
- Purpose: Addresses functional limitations specific to pregnancy
- Coverage: May receive coverage when linked to specific functional goals
Establishing Medical Necessity for Pregnancy Massage
Crucially, insurance companies won’t cover pregnancy massage unless medical necessity gets clearly established. Specifically, “feeling relaxed” or “pregnancy discomfort” doesn’t meet medical necessity standards that payers enforce.
Documentation That Works
Importantly, strong documentation includes:
- Specific functional diagnosis: “Left-sided sciatica radiating down leg, limiting ambulation” rather than just “pregnancy pain”
- Physician referral or prescription specifically requesting therapeutic massage
- Measurable functional goals: “Reduce leg pain 50% to improve sleep quality and daily activity”
- Objective findings: “Palpable myofascial trigger points in left piriformis muscle causing sciatic nerve compression symptoms”
- Treatment response: “Patient reports 40% pain reduction after three sessions; now able to walk 30 minutes versus 10 minutes baseline”
Coverage Varies by Payer Type
Moreover, Medicare explicitly doesn’t cover standalone massage therapy but may cover massage provided by licensed PT/OT as part of their plan of care using CPT code 97140. Furthermore, commercial insurance plans show wide variation. Significantly, some PPO and HMO plans cover 20-30 massage visits annually when prescribed by a physician. However, others exclude massage entirely. Therefore, pre-authorization becomes essential before starting pregnancy massage treatment.
Additionally, Medicaid coverage varies significantly by state. Notably, some states cover massage performed by certified physical or occupational therapists combined with other therapies. Conversely, massage performed alone rarely receives Medicaid coverage. Thus, verify your state’s specific requirements before billing.
Pregnancy Massage Billing Documentation Requirements
What Every Claim Needs
Specifically, successful pregnancy massage claims require:
- Patient demographics and insurance verification
- Physician referral or prescription for therapeutic massage
- Initial assessment documenting functional status and limitations
- Specific treatment plan with measurable goals
- Session notes describing techniques used and outcomes
- Progress notes showing functional improvement
- Periodic re-evaluation documenting ongoing medical necessity
Documentation Transforms Massage Into Billable Treatment
Significantly, many pregnancy massage denials occur not because the service lacks medical value but because documentation fails to establish clear medical necessity. Furthermore, taking thorough notes transforms routine massage into billable medical treatment. Thus, investing time in proper documentation directly impacts claim approval rates and revenue cycle health.
Understanding CPT Code Structure and Organization
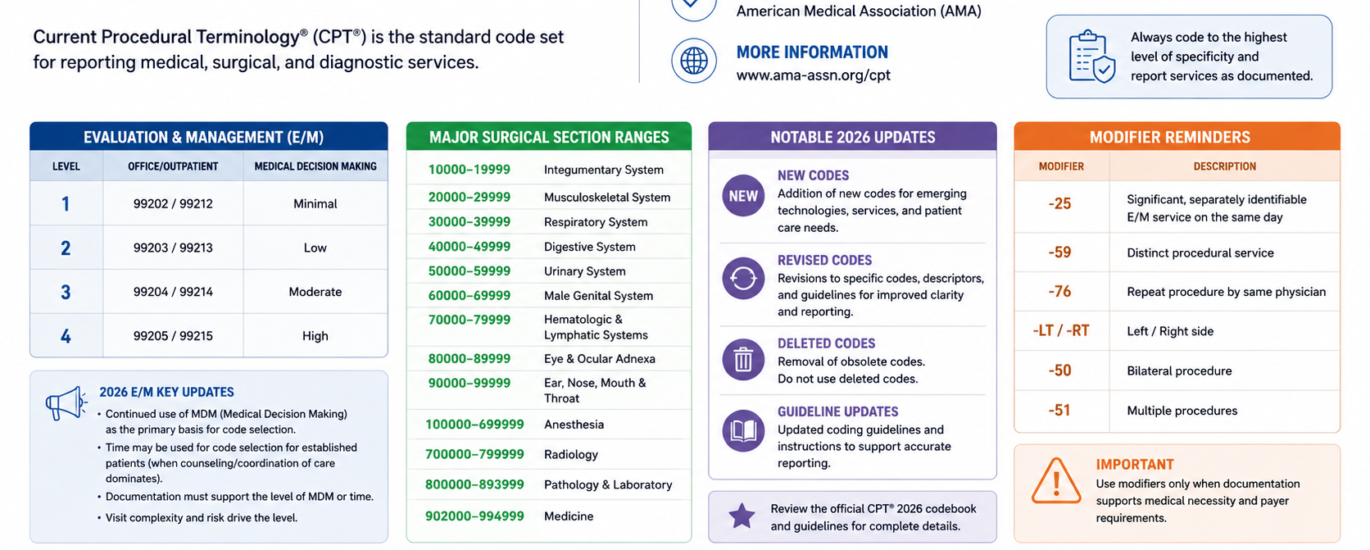
The CPT code set divides into logical sections based on medical specialty:
Evaluation and Management (E/M): Patient visits, consultations, emergency department visits (codes 99200-99607, plus new remote monitoring codes)
Anesthesia: Surgical anesthesia (codes 00100-01999 plus supporting codes)
Surgery: Procedures organized by body system (codes 10001-69990)
Radiology, Nuclear Medicine, Diagnostic Ultrasound: Imaging procedures (codes 70010-79999)
Pathology and Laboratory: Lab tests, tissue analysis (codes 80000-89999)
Medicine Services: Immune globulins, immunizations, therapy (codes 90000-99199)
Category II codes: Performance measures (F-codes, optional)
Category III codes: Emerging services (T-codes, temporary)
Within each section, codes organize mostly numerically. Understanding this structure helps coders navigate the massive code set efficiently.
2026 CPT Code Updates: What Medical Coders Must Know
Medical coders must understand the scope and implications of 2026 changes to remain compliant and avoid billing errors.
AI-Assisted Diagnostic Services
Expanding Use of Artificial Intelligence in Clinical Care
Significantly, the 2026 update substantially expanded codes for AI-driven diagnostics, reflecting artificial intelligence’s growing clinical role in healthcare. Notably, these new codes include:
- 0992T and 0993T: Perivascular fat analysis for cardiac risk assessment
- 0710T: Noninvasive arterial plaque analysis
- 93799: Other emerging cardiovascular services
- 0902T, 0903T-0905T: ECG algorithmic analysis
- 83884: Neurofilament light chain testing
- 82233, 82234, 84393, 84395: Beta-amyloid and tau testing for dementia evaluation
Documentation Requirements for AI Codes
Moreover, these codes validate artificial intelligence as legitimate clinical tool rather than experimental technology. Importantly, documentation must increasingly reflect algorithm involvement, human oversight, and clinical decision-making applied to AI output. Therefore, coders should expect more detailed documentation requirements when billing AI-assisted services.
Remote Patient Monitoring Enhancements
Digital Health Gets Major Updates
Notably, digital health received major attention in 2026 updates, with several new codes:
- 99445: Remote physiologic monitoring device supply (2-15 days in 30-day period)
- 99470: Initial remote patient monitoring treatment management (first 10 minutes, requires real-time interaction)
- 99453, 99454: Revised descriptors for existing RPM codes
Why Time Accuracy Matters
Importantly, these updates acknowledge that effective monitoring doesn’t always require month-long tracking. Furthermore, the time-accuracy emphasis creates critical compliance points for coders. Therefore, understanding these new requirements prevents billing errors and compliance violations.
Lower Extremity Revascularization Redesign
A Major Coding Overhaul
Significantly, perhaps the most dramatic 2026 change involves lower extremity revascularization coding. Notably, approximately 46 new codes replace legacy codes 37220-37235, with new code range 37254-37299. Moreover, the redesign reflects lesion complexity and multiple vascular territories including inframalleolar interventions.
Workflow Implications for Surgical Practices
Therefore, surgical and interventional practices must review how their workflows map to the new structure, ensure accurate lesion-territory documentation, and update charge masters and encoder logic. Additionally, this comprehensive redesign requires significant staff training and system updates.
New Surgical Codes
Expansions Across Multiple Specialties
Moreover, significant additions appear across the surgery section, affecting multiple specialties:
- Biopsy codes: 55707-55715 for prostate biopsy procedures
- Spinal decompression codes: 62330-63032 reflecting new decompression techniques
- Hearing aid services: Complete redesign starting with 92628 for hearing aid candidacy evaluation
- Burn healing classification: Assistive algorithmic classification codes
- Selective enzymatic debridement: New codes for advanced wound care
Radiology and Imaging Updates
Comprehensive Revisions to Imaging Codes
Additionally, the radiology section received substantial revision, with multiple new reporting options:
- 70471-70473: Computed tomographic angiography codes
- 77436-77439: Surface radiation therapy codes
- New codes for CTA of head and neck, CT perfusion studies
- Irreversible electroporation reporting options
Common CPT Coding Mistakes and How to Avoid Them
Understanding the most common coding errors helps you prevent claim denials and maintain compliance. Let’s explore each mistake and its practical solution.
Mistake 1: Incorrect Modifier Application
The Error: Specifically, submitting codes without appropriate modifiers or with wrong modifiers represents a frequent mistake.
The Consequence: Consequently, this error causes claim denials, improper payment amounts, and patient billing issues.
The Solution: Therefore, understanding modifier significance proves essential. Notably, modifier 33 signals preventive services. Furthermore, modifier PT indicates screening-to-therapeutic conversion. Additionally, modifier 59 indicates distinct procedural services performed at different anatomical sites.
Mistake 2: Missing Documentation Support
The Error: Conversely, submitting codes without documentation supporting medical necessity creates compliance vulnerabilities.
The Consequence: Moreover, this omission results in payer denials and audit risks.
The Solution: Importantly, ensure documentation clearly justifies code selection. For pregnancy massage, document specific functional limitations. Additionally, for physical therapy, record complexity factors justifying evaluation tier. Furthermore, for colonoscopy, specify procedure type and interventions performed.
Mistake 3: Bundling Violations
The Error: Furthermore, billing mutually exclusive codes together (example: 45378 plus 45385) violates bundling rules.
The Consequence: Therefore, payers automatically deny these combinations.
The Solution: Ultimately, learn which codes bundle together. Importantly, base codes bundle into therapeutic codes. Additionally, understand the hierarchy. When doubt exists, submit the highest-level therapeutic code performed.
Mistake 4: Skipping Audits and Denial Analysis
The Error: Finally, not monitoring claim denials or analyzing denial patterns creates ongoing revenue loss.
The Consequence: Specifically, this inaction results in repetitive billing errors and missed compliance opportunities.
The Solution: Therefore, run monthly denial reports. Moreover, categorize denial reasons systematically. Additionally, address systemic issues through targeted coder education. Notably, colonoscopies rank among the top 10 most-denied procedures nationally.
Billing Tips for Maximum Reimbursement
Implementing these practical tips significantly improves your claims’ approval rates and revenue cycle health.
Tip 1: Pre-Authorization Prevents Denials
Importantly, request pre-authorization before procedures when required. Notably, pregnancy massage, certain physical therapy sequences, and diagnostic colonoscopies often require advance approval. Therefore, securing pre-auth prevents claim denials and protects practices from unexpected write-offs.
Tip 2: Proper Time Tracking Ensures Accurate Billing
Conversely, physical therapy and massage therapy use time-based codes requiring meticulous attention. Additionally, implement systems ensuring accurate time recording. Importantly, undertracking leaves money on the table. Furthermore, overtracking triggers audits. Therefore, the 8-Minute Rule guides PT billing; coders must fully understand this requirement.
Tip 3: Payer-Specific Knowledge Prevents Headaches
Significantly, different payers enforce different rules. Notably, Medicare uses G-codes for colonoscopy screening. Furthermore, commercial insurers use CPT codes with modifiers. Additionally, Medicaid varies by state. Therefore, maintaining payer-specific reference guides reduces denials significantly.
Tip 4: Complete Documentation Supports Clean Claims
Importantly, incomplete documentation ranks among the top denial reasons. Therefore, before submitting any claim, verify that documentation answers these critical questions:
- What procedure occurred?
- Why was the procedure necessary?
- What specific techniques or interventions happened?
- What were the results?
- What’s the patient’s anatomical extent (for colonoscopy, did scope reach cecum)?
- What complexity level applies (for PT evaluation)?
Documentation Quality Direct ly Impacts Revenue
Specifically, thorough documentation reduces denials, supports audits, and demonstrates proper care. Additionally, it protects coders from compliance issues and keeps the practice’s reputation intact.
Tip 5: Regular Training Keeps Coders Current
Furthermore, CPT codes change annually. Notably, coders need ongoing education covering new codes, revised guidelines, and updated payer policies. Significantly, many top denials result from coders using outdated knowledge. Therefore, investing in regular training prevents far more money than training costs.
FAQs About 2026 CPT Codes for Medical Coders
Medical coders frequently ask these important questions about CPT coding in 2026. Let’s explore the answers in detail.
Q: What’s the difference between CPT code 45378 and G0121 for colonoscopy?
A: Specifically, code 45378 describes diagnostic colonoscopy and gets used for non-Medicare patients or Medicare patients with diagnostic indications. Conversely, G0121 specifically covers colorectal cancer screening for Medicare average-risk patients. Therefore, using the wrong code triggers automatic denials.
Q: Can I bill both 97124 and 97140 in the same session?
A: Only under specific circumstances. Importantly, bill both codes only if you perform massage therapy on one body area and manual therapy on a different area, using modifier 59 to indicate distinct procedural service. Furthermore, billing both codes for the same anatomical area triggers denials.
Q: How do I know which physical therapy evaluation code to select?
A: Notably, review three components: patient history complexity, examination elements addressed, and clinical decision-making required. Furthermore, compare against code descriptors for 97161, 97162, and 97163. Therefore, don’t just default to 97162.
Q: What documentation must I have for pregnancy massage claims?
A: Importantly, gather: physician referral/prescription, specific functional diagnosis, measurable treatment goals, detailed treatment notes describing techniques and outcomes, and periodic re-evaluation confirming medical necessity. Additionally, lacking any of these elements risks claim denials.
Q: What happens if a screening colonoscopy turns therapeutic?
A: The answer varies by payer. For Medicare, use modifier PT with the therapeutic code (example: 45385-PT). Conversely, for commercial insurance, use modifier 33. Therefore, both approaches ensure preventive benefits apply and minimize patient cost-sharing.
Q: Are new 2026 CPT codes mandatory immediately?
A: Absolutely, yes. Notably, effective January 1, 2026, using obsolete codes violates HIPAA compliance requirements. Furthermore, both CMS and private payers automatically reject claims using deleted codes. Therefore, updating your systems immediately matters for compliance.
Q: How does the 8-Minute Rule work for physical therapy?
A: Essentially, coders bill one 15-minute unit for every 8 minutes of treatment time. Specifically, eight minutes minimum equals one unit. Furthermore, sixteen minutes minimum equals two units. Therefore, you’ll accumulate time across timed CPT codes during each session.
Q: What makes a CPT code Category III versus Category I?
A: The key difference involves evidence level. Notably, Category I codes describe established procedures with solid clinical data. Furthermore, Category III codes (T-codes) describe emerging services still accumulating evidence. Therefore, Category III codes may eventually become Category I if sufficient data develops.
Related CPT Codes and Cross-References
Understanding code relationships helps coders select appropriate billing combinations:
Colonoscopy-Related Codes:
- 45330-45398: Flexible endoscopy codes across ranges
- 44388: Colonoscopy through stoma
- G0105, G0121: Screening G-codes
- Anesthesia codes 00812, 00811: When anesthesiologist provides moderate/deep sedation
Physical Therapy Related:
- 97161-97164: All evaluation/re-evaluation codes
- 97110, 97112, 97140, 97530: Treatment procedure codes
- 99453-99454: Remote physiologic monitoring codes
- 99445, 99470: 2026 new remote monitoring codes
Massage and Manual Therapy Related:
- 97124: Therapeutic massage
- 97140: Manual therapy (overlaps with PT codes)
- 97010: Hot/cold packs (mostly bundled now)
- 97530: Therapeutic activities
These cross-references help coders avoid coding multiple services when codes bundle together and help identify when distinct procedural services justify modifier 59.
Conclusion: Mastering CPT Codes in 2026
Importantly, successfully navigating CPT codes for medical billing requires understanding code structure, selecting appropriate codes based on documented services, applying modifiers correctly, and maintaining updated knowledge of annual changes. Significantly, the 2026 CPT update brings substantial changes particularly in AI-assisted services, remote monitoring, and surgical procedures.
Moreover, medical coders holding these competencies protect their practices’ revenue, reduce compliance risk, and ensure patients receive appropriate insurance coverage. Therefore, by mastering the fundamentals covered here, staying current with 2026 changes, and implementing best practices for documentation and payer management, coders position themselves and their organizations for billing success in today’s complex healthcare environment.
Finally, the path to coding excellence involves continuous learning, meticulous documentation, regular denial analysis, and steadfast commitment to accuracy. Significantly, those who invest in these competencies find themselves invaluable to their organizations and better equipped to advance their careers in healthcare’s ever-evolving landscape.