What Is CPT Code 45378: Understanding the Basics
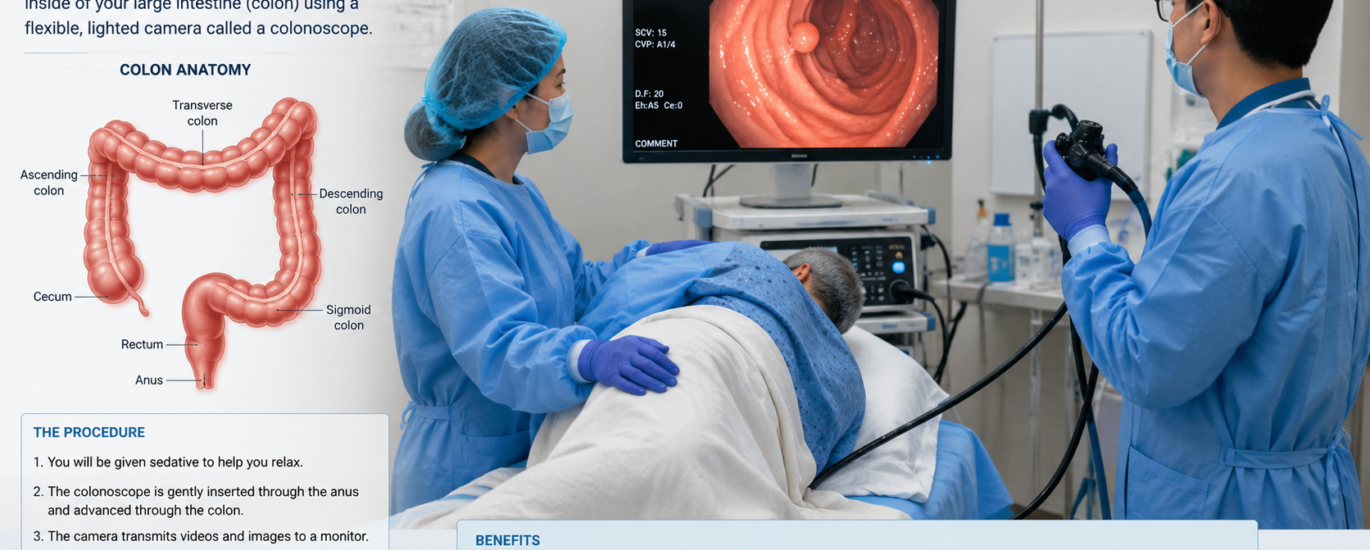
CPT code 45378 represents one of the most frequently used codes in gastroenterology billing, yet many medical coders struggle with its proper application. Specifically, this code describes a diagnostic flexible colonoscopy where a physician examines the entire colon from the rectum to the cecum using a flexible scope.
The official American Medical Association definition states: “Colonoscopy, flexible; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure).” This seemingly simple description actually covers a complex set of rules that every medical coder must understand.
The Difference Between CPT 45378 and Screening Codes
Here’s where confusion often starts. CPT code 45378 is fundamentally different from screening codes like G0105 and G0121. While these G-codes apply exclusively to Medicare patients undergoing preventive colorectal cancer screening, CPT 45378 serves a diagnostic purpose. This distinction matters enormously for billing accuracy and patient cost-sharing.
Think of it this way: screening colonoscopies search for disease in asymptomatic patients, while diagnostic colonoscopies investigate symptoms or abnormal findings. The coding changes dramatically based on this distinction.
Understanding the 45378 CPT Code Description in Detail
The CPT code 45378 description includes several important components that coders must fully comprehend. This code covers a complete diagnostic colonoscopy including:
What’s Included in CPT 45378
The comprehensive visual examination of the entire colon reaches the cecum (or terminal ileum if the cecum was previously removed). The code inherently includes minor diagnostic maneuvers like specimen collection through brushing or washing with saline irrigation. Additionally, minor decompression of the colon qualifies as included work, not separately billable.
Critical: What’s NOT Included
Importantly, CPT code 45378 explicitly excludes any therapeutic interventions. This means if a physician discovers a polyp and removes it, the code changes immediately to a therapeutic code like 45385 (polypectomy using snare technique) or 45380 (biopsy). Billing both codes together triggers automatic claim denials because therapeutic codes bundle the diagnostic work.
This bundling rule represents the most common billing error with CPT 45378. Many practices incorrectly submit both the diagnostic base code and therapeutic codes on the same claim, resulting in denials and lost revenue.
CPT Code for Colonoscopy: Screening vs. Diagnostic
When To Use CPT 45378 for Diagnostic Purposes
You should submit CPT code 45378 when a patient presents with specific symptoms requiring investigation. Common scenarios include:
Patients experiencing rectal bleeding, abdominal pain, chronic diarrhea, or unexplained weight loss need diagnostic evaluation. Additionally, individuals with abnormal findings from other tests (like positive stool-based screening tests) require diagnostic colonoscopy to investigate further. Finally, patients with personal or family history of colorectal issues warrant diagnostic procedures rather than routine screening.
When NOT To Use CPT 45378
Conversely, avoid using CPT code 45378 for Medicare patients undergoing routine screening. Medicare requires using G0105 (for high-risk patients) or G0121 (for average-risk patients) instead. Using 45378 for Medicare screening triggers automatic claim denials—every single time.
For commercial insurance patients, if the colonoscopy serves primarily as screening, bill CPT 45378 with modifier 33. This modifier signals that the primary intent involves delivering preventive care, ensuring proper insurance coverage under the Affordable Care Act.
Screening Colonoscopy ICD 10 Codes and Documentation
ICD-10 Code Selection for Screening
The ICD-10 code you select directly impacts claim approval. For screening colonoscopies, use:
Z12.11 – Encounter for screening for malignant neoplasm of colon
This diagnosis code applies when the colonoscopy’s primary purpose involves colorectal cancer screening in asymptomatic patients. Never use symptom-based diagnosis codes with screening codes, as this creates contradictions that trigger payer denials.
ICD-10 Codes for Diagnostic Indications
Conversely, when billing diagnostic colonoscopy CPT codes, match them with symptom or finding-based ICD-10 codes. Examples include:
K62.5 for hemorrhoids causing rectal bleeding, K59.1 for diarrhea requiring investigation, or R06.02 for abdominal pain necessitating evaluation. The diagnosis code must clearly support the medical necessity of the diagnostic procedure.
Common CPT Code for Screening Colonoscopy Mistakes
Mistake 1: Using 45378 for Medicare Screening
Many coders mistakenly bill CPT 45378 for Medicare screening colonoscopies. This represents a critical error. Medicare explicitly requires G-codes for screening:
G0105 applies to high-risk Medicare patients, while G0121 serves average-risk beneficiaries. Submitting 45378 instead results in automatic denials that damage practice revenue and patient relationships.
Mistake 2: Failing to Use Proper Modifiers
Modifier usage distinguishes clean claims from denials. When a screening colonoscopy converts to therapeutic (polyp removal), different modifiers apply:
Medicare patients require modifier PT (Colorectal cancer screening test converted to diagnostic test or other procedure). This modifier preserves screening preventive benefits while documenting the therapeutic intervention. Omitting PT results in unexpected patient billing.
Commercial insurance patients need modifier 33 (Preventive service) to maintain screening benefits. Forgetting this modifier causes patient billing issues despite the preventive intent.
Mistake 3: Bundling Violations
Never submit CPT 45378 alongside therapeutic codes like 45385 on the same claim. The diagnostic work bundles into therapeutic codes—they’re mutually exclusive. Insurance systems automatically flag this combination and deny payment.
Mistake 4: Incomplete Scope Documentation
Failing to document that the scope reached the cecum creates significant problems. If documentation doesn’t confirm cecal intubation, the procedure downgrades to a flexible sigmoidoscopy code (45330 series), resulting in substantially lower reimbursement.
2026 CPT Code 45378 Updates and Changes
Medicare Coinsurance Policy Update
The 2026 Medicare landscape brings critical changes affecting patient cost-sharing. Specifically, when a Medicare screening colonoscopy converts to therapeutic (such as polyp removal), patients now owe 15% coinsurance from 2023-2026. Notably, deductibles remain waived, but coinsurance applies.
This percentage improves over time: it drops to 10% from 2027-2029, and reaches zero coinsurance by 2030. Patients should understand this before screening procedures to avoid billing surprises.
RVU Values for 2026 Reimbursement
The 2026 Medicare conversion factor of $33.40 means CPT 45378 generates approximately $112 in reimbursement (3.36 work RVU multiplied by conversion factor). Therapeutic codes generate higher reimbursement: 45380 (biopsy) yields $122.60, while 45385 (snare polypectomy) generates $152.74.
Understanding these values helps practices evaluate productivity and validate compensation arrangements with physicians.
New Documentation Requirements
As of 2026, payers increasingly scrutinize documentation. Specifically, record whether the scope reached the cecum, specimen collection methods used, and detailed descriptions of any findings. Comprehensive documentation prevents audits and supports claim approval.
Diagnostic Colonoscopy CPT Code Billing Tips
Tip 1: Verify Payer Guidelines Before Billing
Different insurance companies enforce different rules. Medicare requires specific G-codes, while commercial insurers often accept CPT codes with appropriate modifiers. Verify your patient’s insurance and apply the correct code before submitting claims.
Tip 2: Document Medical Necessity Thoroughly
Each diagnostic colonoscopy claim requires supporting documentation showing why the procedure was medically necessary. Include presenting symptoms, abnormal findings from prior tests, or relevant patient history. Insufficient documentation triggers denial letters and resubmission delays.
Tip 3: Use Proper Modifiers Every Time
Modifiers communicate critical information to payers. Modifier 33 preserves preventive benefits for commercial screening. And Modifier PT documents screening-to-therapeutic conversion for Medicare. Modifier 53 indicates discontinued procedures when the scope couldn’t reach the cecum. Missing modifiers cause claim complications.
Tip 4: Confirm Scope Completion
Before submitting claims, verify documentation clearly states the scope reached the cecum or terminal ileum. If documentation indicates the scope only reached the sigmoid colon due to poor preparation or patient tolerance, use appropriate sigmoidoscopy codes instead. Incorrect codes trigger denials.
Related CPT Codes for Colonoscopy Procedures
Understanding the full colonoscopy code range prevents coding errors. CPT codes 45378-45398 cover the colonoscopy spectrum:
45378 serves diagnostic colonoscopy without intervention. 45379 applies when foreign bodies require removal. 45380 covers biopsy procedures, while 45385 describes snare polypectomy. 45390 indicates endoscopic mucosal resection (advanced polypectomy). 45391-45392 cover endoscopic ultrasound procedures. 45389 describes stent placement within the colon.
Each code represents different complexity levels and reimbursement amounts. Selecting the highest-level code matching actual procedures ensures maximum appropriate reimbursement.
Meaning and Application of CPT 45378
The meaning of CPT code 45378 centers on diagnostic examination without therapeutic intervention. Physicians use this code when they examine the colon to investigate symptoms, evaluate abnormal findings, or screen high-risk patients. The procedure includes specimen collection through brushing or washing but excludes treatment.
This fundamental concept—diagnostic without therapeutic—drives all 45378 coding decisions. When therapeutic work occurs, the code changes. When Medicare screening occurs, G-codes apply instead. When proper modifiers aren’t used, claims face denial.
Causes and Indications for CPT 45378 Use
Medical professionals order diagnostic colonoscopies (billed with CPT 45378) for several specific reasons:
Primary Indications
Rectal bleeding or blood in stool requires colonoscopy evaluation to identify sources. Chronic diarrhea lasting weeks warrants investigation to rule out inflammatory bowel disease or infection. Unexplained weight loss suggests possible GI pathology requiring colonoscopic evaluation. Abdominal pain, particularly when persistent, often necessitates diagnostic colonoscopy.
Additionally, abnormal findings from non-invasive stool testing (like positive FIT or Cologuard results) trigger diagnostic colonoscopy. Patients with strong family histories of colorectal cancer may need earlier diagnostic screening beyond standard age-based recommendations.
Secondary Indications
Surveillance colonoscopies for patients with prior polyp history follow-up findings from CT imaging or other imaging studies. Additionally, evaluation of possible inflammatory bowel disease manifestations requires diagnostic colonoscopy.
FAQ:
Q: Can I bill 45378 with 45385 on the same claim?
A: No. This represents a critical bundling violation. The therapeutic code (45385) includes the diagnostic work, making 45378 separately reportable. Payers automatically deny this combination. Always submit only the highest-level therapeutic code performed.
Q: What’s the difference between 45378 and G0121?
A: CPT 45378 serves diagnostic indications and applies to non-Medicare patients or Medicare patients with symptoms. G0121 covers Medicare screening for average-risk patients. Using 45378 for Medicare screening triggers denials; always verify the patient’s insurance and indication before code selection.
Q: Should I add modifier 33 to Medicare 45378 claims?
A: No. Modifier 33 applies to commercial insurance patients only. Medicare uses G-codes for screening, not CPT 45378. Adding modifier 33 to Medicare claims confuses payer systems and triggers denials or payment delays.
Q: What ICD-10 code pairs with screening colonoscopy 45378?
A: Use Z12.11 (Encounter for screening for malignant neoplasm of colon) for screening indications. For diagnostic colonoscopy, use symptom-based codes like K62.5, K59.1, or R06.02 depending on presenting symptoms.
Q: What happens if the scope doesn’t reach the cecum?
A: Documentation becomes critical. If the scope reached the splenic flexure, you can still use 45378 with modifier 53 (discontinued procedure). If the scope only reached the sigmoid colon, downgrade to sigmoidoscopy codes (45330 series). Always document why scope advancement stopped (patient intolerance, poor preparation, obstructing lesion).
Q: Are anesthesia services billed separately with 45378?
A: Yes. If the endoscopist provides moderate sedation, bill anesthesia code 99152 separately. If an anesthesiologist administers deep sedation (Propofol), they bill 00812 or 00811. Never bundle anesthesia with the procedure code.
Q: How do I code a screening colonoscopy that finds and removes a polyp?
A: The code changes immediately to the therapeutic code (usually 45385 for snare polypectomy). For Medicare patients, append modifier PT. For commercial patients, append modifier 33. The therapeutic code supersedes the screening code.
Summary: Mastering CPT Code 45378 in 2026
CPT code 45378 requires careful attention to detail, proper modifier selection, and thorough documentation. This code distinguishes itself from screening codes through its diagnostic focus and therapeutic exclusions. Understanding these nuances prevents costly billing errors and maintains revenue cycle efficiency.
Medical coders who master CPT 45378 application—including bundling rules, modifier protocols, and ICD-10 coordination—position their practices for billing success. Staying current with 2026 Medicare coinsurance changes, RVU values, and documentation requirements ensures compliance while maximizing appropriate reimbursement. The time invested in thoroughly understanding this commonly used code pays dividends through improved claim approval rates and reduced denials.