

What Is Modifier 25? The Definition You Actually Need
If you work in medical billing, coding, or practice management, you have heard of modifier 25 more times than you can count. And yet, it keeps showing up on audit radar screens across the country. So let us start at the very beginning and get the modifier 25 description crystal clear.
The official modifier 25 definition, as established by the American Medical Association (AMA), states:
Modifier 25 = A significant, separately identifiable evaluation and management (E/M) service performed by the same physician or other qualified healthcare professional on the same day as another procedure or other service.
In plain English, when a provider sees a patient and performs both an E/M service (an office visit, a new patient evaluation, a follow-up assessment) AND a separate procedure on the same calendar day, modifier 25 gets added to the E/M code. This signals to the payer that those two services are genuinely distinct and both deserve reimbursement.
Modifier 25 is appended to the E/M code only, never to the procedure code. That is a fundamental rule. The 25 modifier lives on the visit code, and the procedure code stands on its own without it.
The Phrase That Makes or Breaks Your Claim
The key phrase in the entire 25 modifier definition is “separately identifiable.” That is the phrase that wins or loses the claim. The E/M service has to stand completely on its own. Simply put, if you strip the procedure out of the visit, the E/M service must still hold up as a legitimate, medically necessary encounter all by itself.
Why Modifier 25 Exists in the First Place
To really understand when and how to use modifier 25 correctly, you first need to understand why it exists.
Every CPT procedure code already includes a built-in allowance for pre-service and post-service work. When a provider performs a procedure, CMS and payers assume the provider evaluated the patient beforehand, explained the procedure, and monitored them briefly afterward. That evaluation work is considered “bundled” into the procedure’s reimbursement, so payers will not pay separately for it.
The Classic Bundling Problem
Here is where the real issue shows up. A patient comes in for a scheduled skin biopsy. While the provider examines the patient before the biopsy, they notice the patient’s blood pressure is dangerously high and spends the next 20 minutes evaluating, adjusting medications, and counseling the patient about hypertension. That is a completely separate clinical issue with nothing to do with the biopsy.
Without modifier 25, the payer’s computer would automatically bundle that office visit into the biopsy payment and reject the E/M charge. Essentially, modifier 25 is how the provider says to the payer: “Wait. That visit was real, separate, and medically necessary. Pay it.”
That is the entire purpose of the 25 modifier.
When to Use Modifier 25: Real-World Scenarios
Understanding the modifier 25 description is one thing. Knowing exactly when to reach for it in practice is another. Here are the most common and legitimate use cases:
Preventive Visit Plus a New Problem
A patient schedules an Annual Wellness Visit (AWV). During the exam, they mention new chest tightness. The provider spends additional time evaluating the symptom, orders an EKG, and starts a workup. The AWV gets billed using the appropriate HCPCS code, and the E/M service for the chest pain evaluation gets modifier 25 appended to it.
Chronic Condition Follow-Up Plus a Minor Procedure
A patient comes in for a routine diabetes management follow-up. The provider also notices a suspicious lesion and performs a shave removal during the same visit. The office visit for diabetes management gets modifier 25 applied, alongside the procedure code for the lesion removal.
Established Patient With an Unrelated Acute Issue Plus a Procedure
A patient is in for a scheduled joint injection. While there, they bring up a new problem — say, a painful rash that has been spreading. The provider separately evaluates the rash, prescribes treatment, and documents a distinct clinical assessment. As a result, the E/M for the rash evaluation gets modifier 25, and the injection code stands alone.
Mental Health Visit Plus Physical Procedure
Less common but still valid: a psychiatrist managing a patient’s medication performs a minor procedure (such as a long-acting injectable medication administration) and also conducts a full psychiatric evaluation. When the evaluation goes beyond routine pre-injection assessment, modifier 25 is appropriate.
The test in every scenario is always the same: Does the E/M service stand alone as a separate, billable visit independent of the procedure? If yes, use the 25 modifier. If no, do not.
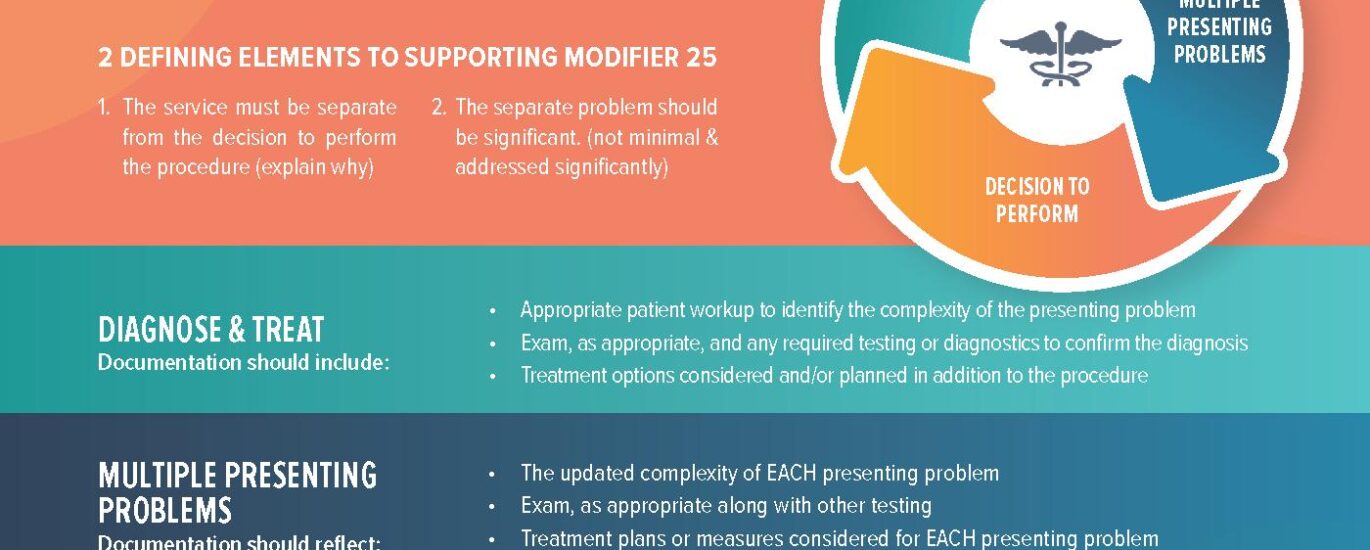
Modifier 25 Description: What the Documentation Must Show
Here is where most practices fall apart. Getting the modifier 25 definition right conceptually is not enough. The clinical documentation has to back it up every single time.
According to Medicare Administrative Contractor (MAC) guidance, a properly documented E/M service must include its own history, examination, and medical decision-making (MDM). These elements must be clearly documented and visibly distinct from any pre-procedure evaluation in the same note.
The Modifier 25 Documentation Checklist
A practical checklist for modifier 25 compliance covers four key areas:
Chief Complaint for the E/M: The note must clearly state a separate reason for the E/M visit. Referencing only the procedure being performed is not sufficient.
Separate Assessment and Plan: The A/P section must address the E/M-related condition independently. When the note’s entire assessment only references the procedure, there is no defensible E/M.
Medical Decision-Making: The MDM for the E/M must demonstrate clinical complexity appropriate to the level of E/M code being billed. Billing a 99214 means the MDM documentation needs to support that level, completely separate from any MDM related to the procedure.
Distinct Documentation Section: Ideally, the procedure note and the E/M note appear as clearly labeled, distinct sections within the medical record. When payers request records for audits, muddled notes that blend the procedure and the E/M together almost always result in a denial or recoupment.
Why Copy-Paste Templates Are a Liability
Providers who rely on copy-paste templates or system-generated notes are especially vulnerable here. Technology is only as good as its programming, and a note template that auto-populates the same boilerplate for every encounter simply will not hold up in an audit. Structured, encounter-specific documentation is the only real protection.
Billing Tips for Modifier 25 in 2026
Getting the modifier 25 workflow right means following a few non-negotiable billing practices. After working in this space for years, these are the tips that actually move the needle:
Tip 1: Always Apply the Stand-Alone Test First
Before appending modifier 25 to any claim, every coder and biller should mentally run the stand-alone test. Ask yourself: if the procedure did not happen today, would the E/M visit still be justified? When the honest answer is yes, proceed with modifier 25. If the answer is “not really,” the E/M is already bundled into the procedure.
Tip 2: Build Modifier 25-Ready Documentation Templates
Work with your providers to create EHR note templates that include a clearly labeled E/M section separate from the procedure section. Providers who document in structured templates that naturally separate the visit from the procedure give your claims the best possible defense.
Tip 3: Run a Modifier 25 Denial Analysis Every Month
Pull a report of all modifier 25 claims and their outcomes every 30 days. When denial rates start climbing, you have an early warning signal to investigate before it becomes a full audit. Track which providers, which procedures, and which payers are generating the most friction.
Tip 4: Train Clinical Staff, Not Just Billing Staff
Modifier 25 compliance starts in the exam room, not the billing department. Providers need to understand that their documentation style directly drives reimbursement outcomes. A focused 15-minute training session with clinical staff — centered on why the E/M note needs to clearly stand apart from the procedure note — pays off immediately.
Tip 5: Know Your Payer Policies
While CMS establishes the general rules, commercial payers sometimes impose stricter requirements around modifier 25 usage. Some payers cap the frequency of same-day E/M and procedure billing, and others require prior authorization for specific procedure codes billed with a 25 modifier. Always verify payer-specific policies, especially for high-volume procedures in your specialty.
Tip 6: Flag High-Risk Procedure Categories
Certain procedures consistently draw extra scrutiny when paired with modifier 25. Eye injections, minor dermatology procedures, joint injections, and preventive visits are the categories where audit attention is highest. In these areas, extra documentation rigor is not optional — it is a matter of survival.
Related Codes and Modifiers You Need to Know
Modifier 25 does not exist in isolation. It works alongside a broader set of coding tools, and understanding those relationships helps you code more accurately and avoid compliance pitfalls.
Modifier 59 vs. Modifier 25
Often confused with modifier 25, Modifier 59 signals that a procedure is distinct from another procedure performed on the same day. While modifier 25 explains a separate E/M service, modifier 59 handles procedure-to-procedure separation. These two modifiers serve completely different purposes and should never be used interchangeably. Mixing them up is one of the top triggers for OIG audit activity.
X Modifiers: XE, XS, XP, XU
In 2026, Medicare and many commercial payers increasingly prefer the more specific X modifiers over the broad modifier 59. XE signals a separate encounter, XS indicates a separate anatomical structure, XP reflects a separate practitioner, and XU applies when the service is unusual and not overlapping with the primary service.
G2211 Complexity Add-On Code
This one is especially critical in 2026. CMS guidance makes clear that when a procedure is performed during the same encounter and modifier 25 is appended to the E/M code, G2211 generally cannot be billed on that same day. Payer systems are now actively programmed to deny G2211 whenever modifier 25 appears on the claim.
Modifier 57: Decision for Surgery
Modifier 57 applies when the E/M service — during which the decision to perform a major surgical procedure was made — occurs on the same day as the surgery. It is specifically for major procedures with 90-day global periods and is entirely distinct from modifier 25, which handles minor or zero-day global procedures.
Common E/M Codes Paired With Modifier 25
CPT codes 99213, 99214, and 99215 are the office visit E/M codes most frequently paired with modifier 25 in outpatient settings. Regardless of the procedure performed on the same day, the level of service must be fully supported by the documentation.
Common Mistakes Coders and Providers Make With Modifier 25
These are the mistakes showing up in real-world audits and denial queues right now. Avoid every single one of them.
Mistake 1: Treating Modifier 25 as a Routine Bypass Code
The most dangerous misconception in medical billing is treating modifier 25 as a way to automatically bill an E/M alongside every procedure. Some coders append it reflexively whenever a procedure appears on a claim without ever reviewing the documentation. This is exactly the behavior that triggers OIG investigations.
Mistake 2: Vague or Blended Documentation
When the provider’s note reads like one continuous clinical encounter where the procedure evaluation and the E/M blur together, there is no way to defend both charges. Clear delineation between the two services is non-negotiable.
Mistake 3: Using Modifier 25 for the Pre-Procedure Evaluation
The evaluation a provider performs to determine that a procedure is needed — and to counsel the patient — is already included in the procedure code’s reimbursement. Billing separately for routine pre-procedure evaluation by appending modifier 25 is both a coding error and a compliance violation.
Mistake 4: Applying Modifier 25 to the Procedure Code
Basic as it sounds, this error still happens. Modifier 25 goes on the E/M code, not the procedure code. Full stop.
Mistake 5: Ignoring Payer-Specific Edits
Medicare’s NCCI (National Correct Coding Initiative) edits bundle many procedure codes with E/M services. Modifier 25 can override some of these edits, but not all of them. Checking NCCI edits before billing is a necessary step, not an optional one.
Mistake 6: Billing Modifier 25 With G2211 Together
CMS guidance for 2025 and continuing into 2026 is clear on this point. When modifier 25 appears on an E/M code billed alongside a procedure, G2211 is not allowed on the same claim. Many practices learned this the hard way after October 2024, when payer systems began auto-denying G2211 in this combination.
Mistake 7: Letting Technology Make the Decision
EHR systems and billing software often flag opportunities to append modifier 25. However, a software edit is a suggestion, not a clinical or compliance decision. Every modifier 25 application still requires a human review of the documentation to confirm the E/M is genuinely distinct.
2026 Updates: What Changed for Modifier 25 This Year
The 2026 billing environment has raised the stakes around modifier 25 in several important ways.
G2211 Conflict Now Formalized in Payer Systems
CMS’s guidance on the incompatibility of modifier 25 and G2211 on the same claim has been fully absorbed into payer system edits across Medicare and most commercial carriers. Practices that have not updated their claim scrubbing rules to catch this combination are already seeing automatic denials.
Increased OIG Audit Focus on Same-Day Billing
The Office of Inspector General’s most recent work plan confirms that E/M services billed same-day with procedures remain a high-priority audit target. A previously published OIG report reviewed 24 sampled E/M claims billed with modifier 25 alongside eye injections and found that 22 of them did not support the modifier’s use. That is a 91% non-compliance rate in that sample. Financially, the same audit identified roughly 124 million dollars in potentially improper Medicare payments for that procedure category alone.
Data-Driven Payer Auditing Is Here
Payers are now using machine learning and pattern recognition tools to identify providers whose modifier 25 billing frequency exceeds peer benchmarks. When your practice’s modifier 25 rate is statistically higher than similar practices in your specialty and region, you land on a watchlist whether you know it or not.
Provider Self-Coding Carries New Risks
A growing number of health systems have shifted to having providers code their own clinical visits rather than routing them through dedicated coding departments. While this can improve efficiency, it also increases the risk of inappropriate modifier 25 use. Providers often append it reflexively based on software prompts rather than through genuine coding analysis.
Compliance Programs Are Now Expected, Not Optional
In 2026, CMS increasingly expects practices billing at high modifier 25 frequencies to maintain documented internal compliance programs. These include periodic self-audits, coder education records, and denial tracking logs. Having a compliance program on paper but not in practice offers little protection when an auditor shows up.
FAQ:
Q: What is modifier 25 in simple terms?
A: Modifier 25 tells an insurance payer that the provider performed a real, separate office visit on the same day as a procedure. Both services deserve separate payment because they addressed different clinical issues.
Q: What is the official modifier 25 description?
A: The AMA defines it as a “significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service.”
Q: When should you NOT use modifier 25?
A: Avoid modifier 25 when the E/M visit is simply the pre-procedure evaluation already bundled into the procedure code. Equally important, skip it when the documentation does not clearly support a distinct and separate clinical encounter.
Q: Can modifier 25 and G2211 be billed together in 2026?
A: In most cases, no. Current CMS guidance specifies that when modifier 25 is appended to an E/M service billed alongside a procedure with a 0-day global period, G2211 cannot also appear on the same claim. Most payer systems now automatically deny G2211 in this context.
Q: Does modifier 25 require a different diagnosis code?
A: A different diagnosis code for the E/M and the procedure strongly supports modifier 25 and makes the claim much easier to defend. In some cases, the same diagnosis can justify both services. Ultimately, the documentation of why the E/M was separately necessary is what matters most.
Q: What is the difference between modifier 25 and modifier 57?
A: Modifier 25 applies when a separate E/M is performed on the same day as a minor procedure with a 0-day global period. Modifier 57, on the other hand, applies when the E/M service is the visit during which the decision to perform a major surgical procedure (90-day global period) was made.
Q: Can modifier 25 be used with any CPT code?
A: No. Modifier 25 is appended to E/M CPT codes only. It does not belong on procedure codes, lab codes, radiology codes, or any other service category.
Q: Does modifier 25 guarantee payment?
A: Absolutely not. The modifier signals the intent that the E/M is separately payable, but the payer will still review the documentation. Without a distinct and defensible E/M in the clinical notes, the claim will be denied regardless of the modifier.
Q: How often do claims with modifier 25 get audited?
A: Modifier 25 is the single most audited modifier in medical billing. Payers, RAC auditors, MAC contractors, and the OIG all routinely target high-frequency modifier 25 billers for post-payment review.
The Bottom Line on Modifier 25
When you truly understand the 25 modifier definition and apply it with precision and solid documentation, it becomes one of the most valuable tools in your billing arsenal. Used correctly, it protects legitimate revenue and ensures providers get paid for real clinical work they actually performed.
Careless use, however, tells a completely different story. Treating it as a shortcut or a routine add-on to any procedure claim is the fastest path to audits, recoupments, and compliance headaches. In 2026, with payer analytics more sophisticated than ever and OIG scrutiny at an all-time high, the margin for sloppiness is basically zero.
Get the documentation right. Train your clinical staff. Build the stand-alone test into your daily workflow. Above all, treat every modifier 25 claim as if an auditor is going to read that note next week. Because sometimes, they actually will.
This article is written for educational and informational purposes for healthcare coders, billers, and practice management professionals. Always refer to the most current CMS guidelines, your MAC’s local coverage policies, and the AMA’s CPT coding resources for authoritative coding guidance. your MAC’s local coverage policies, and the AMA’s CPT coding resources for authoritative coding guidance.




