

What Is the ICD-10 Code for Multiple Sclerosis?
If you work in medical billing, neurology coding, or healthcare administration, you already know that getting the diagnosis code right is everything. And in 2026, the rules around the ICD-10 code for multiple sclerosis changed in a pretty big way.
For years, every single MS patient, regardless of their type or disease activity, got slapped with the same code: G35. That was it. One code for all of it. But starting October 1, 2025, that old single-code approach is gone. The ICD-10 MS coding system has expanded into specific subcategories, and if you are still using the standalone G35 on claims for dates of service after that cutoff, your claims are getting rejected. Plain and simple.
So let us break this all the way down, covering what the new codes mean, how to use them correctly, what MS actually is, what the symptoms look like, and what you absolutely need to avoid in your billing workflow.
What Is Multiple Sclerosis? (The Meaning Behind the Diagnosis)
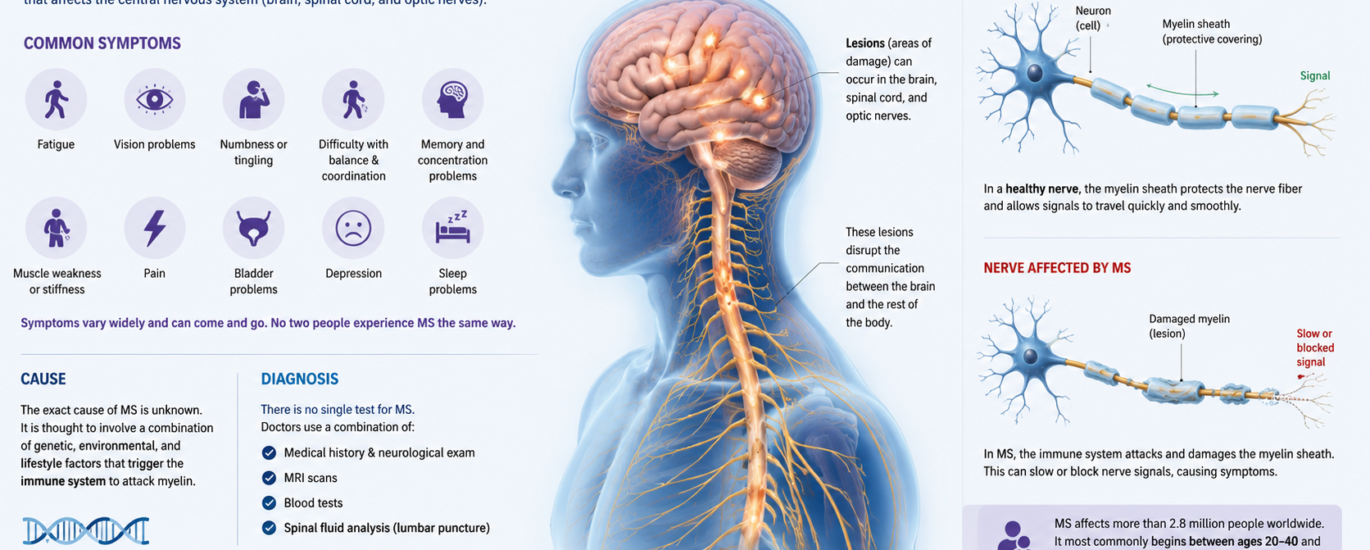
Before diving into the codes, it is worth actually understanding what we are coding for. Multiple sclerosis, or MS, is a chronic autoimmune disease that attacks the central nervous system, meaning the brain and spinal cord. Basically, the body’s own immune system goes rogue and starts destroying myelin, which is the protective coating around nerve fibers. When that coating breaks down, nerve signals slow down or stop completely.
Think of it like a power cord with frayed insulation. The electricity (nerve signal) can not travel properly, so you get short circuits in the form of symptoms.
MS is not rare. It affects more than 2.9 million people worldwide, and in the United States alone, nearly one million people live with a diagnosis. It shows up most commonly in adults between the ages of 20 and 40, and women are diagnosed nearly three times more often than men.
There is no cure. But with the right treatment, disease-modifying therapies, and rehabilitation, many people manage their symptoms and maintain a good quality of life.
Symptoms of Multiple Sclerosis
MS symptoms vary wildly from person to person. That is actually part of what makes it so tricky to diagnose and document. The location of the damaged nerve tissue in the brain or spinal cord determines what symptoms show up.
Here are the most commonly reported ones:
Physical Symptoms:
- Fatigue (the most common and often most disabling symptom)
- Muscle weakness, especially in the legs
- Problems with balance and coordination
- Numbness or tingling in the arms, legs, or face
- Muscle spasms and stiffness (spasticity)
- Trouble walking or gait problems
- Vision problems, including blurred or double vision (optic neuritis is frequently the first sign)
- Bladder and bowel dysfunction
- Dizziness and vertigo
Cognitive and Emotional Symptoms:
- Memory problems and difficulty concentrating (sometimes called “cog fog”)
- Slowed thinking and processing speed
- Depression and anxiety
- Mood swings
During a relapse, also known as a flare-up, symptoms either suddenly appear or get dramatically worse. When it comes to coding an ICD-10 MS flare, you now have to specify the disease type and its activity status, which we will cover below.
Causes of Multiple Sclerosis
Nobody knows exactly what causes MS. That is the honest answer. Researchers believe it is a combination of genetic predisposition and environmental triggers that set off the immune system’s attack on myelin.
The major contributing factors include:
Genetic factors: Having a first-degree relative with MS raises your risk. However, MS is not purely hereditary. Even identical twins show only about a 25% concordance rate.
Environmental triggers: Low vitamin D levels, Epstein-Barr virus (EBV) exposure, and smoking have all been associated with higher MS risk. A 2022 study from Harvard strongly linked prior EBV infection to MS development.
Geographic patterns: MS is far more common in regions far from the equator. People living in northern climates, where sunlight exposure and therefore vitamin D production is lower, tend to have higher rates.
Gender and hormones: Women are significantly more prone to MS. Hormonal influences likely play a role, though the exact mechanism is still being studied.
Understanding the cause matters for clinical documentation. When you code MS in 2026, insurance payers want specificity about what type of MS the patient has, not just a vague diagnosis.
The 2026 G35 ICD-10 Code Update: What Actually Changed
Here is the centerpiece of everything you need to know right now.
The old standalone G35 ICD-10 code for multiple sclerosis is officially retired for billing purposes as of October 1, 2025. As of the FY 2026 ICD-10-CM update, G35 is now a parent code that contains a family of new subcategory codes. Each one captures the specific MS subtype and, importantly, whether the disease is currently active or not.
This is not just a minor update. This is one of the largest conceptual shifts in neurological coding in years. And if your billing team has not updated their charge master, EHR templates, or coding workflows, you are already behind.
Here is the full breakdown of the new 2026 MS codes:
G35.A — Relapsing-Remitting Multiple Sclerosis (RRMS)
This is the most common form of MS, accounting for roughly 85% of initial diagnoses. Patients with RRMS experience clearly defined relapses (attacks of worsening symptoms) followed by periods of partial or complete recovery. When coding an ICD-10 MS flare in this population, G35.A is your code. There is no active/inactive distinction for RRMS in the current structure; the relapsing nature is inherent to the subtype.
G35.B — Primary Progressive Multiple Sclerosis (PPMS)
PPMS is characterized by steady worsening neurological function from the very start, without distinct relapses or remissions. It affects about 10 to 15 percent of MS patients. The G35.B subcategory breaks down further:
- G35.B0 — Primary progressive MS, activity unspecified
- G35.B1 — Active primary progressive MS (new MRI lesions, clinical relapse signs)
- G35.B2 — Non-active primary progressive MS (stable, no new activity)
G35.C — Secondary Progressive Multiple Sclerosis (SPMS)
SPMS occurs when a patient originally diagnosed with RRMS transitions to a phase of steady progressive decline without clear relapses. This typically happens after 10 to 20 years. The G35.C subcategory also carries activity distinctions:
- G35.C0 — Secondary progressive MS, activity unspecified
- G35.C1 — Active secondary progressive MS
- G35.C2 — Non-active secondary progressive MS
G35.D — Multiple Sclerosis, Unspecified
This is the catch-all when the subtype is genuinely not documented. But be careful here. Using G35.D because documentation is vague invites payer scrutiny. Coders should always query the provider to get the specific MS type before defaulting to unspecified.
Multiple Sclerosis ICD-9 vs ICD-10: A Quick Historical Note
For any coders or billers who remember working with the ICD-9 system, multiple sclerosis was coded as 340 under the ICD-9-CM classification. That system was retired in October 2015 when the U.S. transitioned to ICD-10-CM. Under ICD-10, everything moved to the single G35 code, which has now, in 2026, expanded into the subcategory structure described above.
If you encounter any historical records or crosswalk documentation that references multiple sclerosis ICD-9 code 340, just know it maps to the G35 family in the current system.
Related ICD-10 Codes You Should Know
Multiple sclerosis rarely comes to a billing encounter alone. Patients often present with a range of comorbidities and complications that need their own codes. Here are the most frequently paired codes:
- G35.A, G35.B_, G35.C_, or G35.D — The primary MS code (always first on the claim)
- R53.83 — Fatigue (a near-universal MS symptom)
- G35 + F32.x — Depression comorbid with MS
- N39.3 — Stress urinary incontinence (bladder dysfunction in MS)
- G82.xx — Paraplegia or paraparesis for significant motor involvement
- H46.x — Optic neuritis (a common early MS symptom)
- G37.3 — Acute transverse myelitis (sometimes associated with MS)
- Z79.899 — Other long-term drug therapy (relevant for disease-modifying therapies like natalizumab or ocrelizumab)
Always code all documented conditions relevant to the encounter. More complete coding supports better risk adjustment and reduces the chance of a payer audit.
Billing Tips for Multiple Sclerosis in 2026
Getting the ICD-10 ms code right is not just about avoiding rejections. It directly affects reimbursement rates, risk adjustment scoring, and your practice’s quality metrics. Here are the most important billing tips for MS in 2026:
1. Always document the MS subtype in the clinical note. This is the number-one requirement. Payers will not accept vague language like “patient has MS.” The note must specify whether the patient has relapsing-remitting MS, primary progressive MS, or secondary progressive MS.
2. Document disease activity status. For primary and secondary progressive MS codes, you need to specify whether the disease is active or non-active. Active MS means there are new lesions on MRI, a clinical relapse, or new symptoms. Non-active means the disease is currently stable with no new indicators of progression.
3. Stop using standalone G35. As of October 1, 2025, claims submitted with only G35 (no subcategory) for MS encounters are subject to rejection. The payer systems are already updated.
4. Query your providers proactively. If the documentation does not specify the subtype, the coder must query the neurologist before submitting the claim. Building a standardized query template into your workflow saves time and prevents denials.
5. Update your EHR drop-down lists. Many practices discovered in October 2025 that their EHR systems were still defaulting to G35 without presenting subcategory options. Work with your IT or EHR vendor to ensure the new code tree is fully activated.
6. Review MS-related DRGs. MS encounters fall within MS-DRG v43.0 groups 058, 059, and 060. These cover MS and cerebellar ataxia with major complications (MCC), complications (CC), and without CC or MCC respectively. Accurate comorbidity coding determines which DRG the claim lands in.
Common Coding Mistakes to Avoid
Even experienced coders are tripping over these right now:
Mistake #1: Using G35 alone after October 1, 2025. This is the big one. G35 by itself is no longer a valid billable code. Always use a subcategory.
Mistake #2: Defaulting to G35.D (unspecified) without querying the provider. G35.D exists for genuine uncertainty, not coder convenience. Overuse of unspecified codes can trigger payer audits and quality flag concerns.
Mistake #3: Not capturing disease activity in progressive MS. Coding G35.B or G35.C without specifying the 0/1/2 modifier (unspecified, active, non-active) is incomplete. Use the full code.
Mistake #4: Missing comorbidities. If the neurologist documents fatigue, bladder dysfunction, or depression related to MS, those conditions need their own codes on the claim. Missing them means missed reimbursement opportunity.
Mistake #5: Using ICD-9 code 340 on any current claim. ICD-9 has been dead since 2015. If it is showing up somewhere in your system, you have a bigger workflow problem to address.
Mistake #6: Confusing MS with related demyelinating conditions. Neuromyelitis optica spectrum disorder (NMOSD), acute disseminated encephalomyelitis (ADEM), and other conditions have their own separate codes. Do not code them as MS without explicit provider documentation.
2026 Updates: What Is New This Year
The FY 2026 ICD-10-CM update, effective October 1, 2025, brought the following significant changes for multiple sclerosis coding:
G35 restructured into subcategories: As detailed above, the single G35 code is now a parent with subcategory codes for each MS phenotype. This is the most impactful neurological coding change of the year.
Activity status required for progressive subtypes: For the first time, coders must document and capture whether progressive MS is currently active or non-active. This specificity supports more precise risk adjustment and treatment planning.
487 total new ICD-10-CM codes: The full FY 2026 update includes 487 new codes across all specialties, 38 revisions, and 28 deletions. MS saw one of the largest single-category expansions in the entire update cycle.
CMS officially recognizes MS subtypes for quality reporting: The new subcategory structure aligns with Medicare quality programs, making accurate MS subtype coding directly relevant to value-based care performance metrics.
EHR and clearinghouse readiness: Any practice that had not updated its systems by October 1, 2025 experienced a wave of denials. If you are catching up now, prioritize your EHR template updates and staff retraining immediately.
FAQ: ICD-10 Code for Multiple Sclerosis
Q: What is the main ICD-10 code for multiple sclerosis in 2026?
A: G35 is the parent code, but you must use a subcategory for billing. The main subcategories are G35.A (relapsing-remitting), G35.B (primary progressive), G35.C (secondary progressive), and G35.D (unspecified).
Q: Is G35 still a valid ICD-10 code in 2026?
A: G35 is now a parent category code, not a valid standalone billing code for dates of service on or after October 1, 2025. Using only G35 without a subcategory will result in a claim rejection.
Q: What is the ICD-10 code for an MS flare or relapse?
A: An ICD-10 MS flare in a relapsing-remitting patient is coded as G35.A. For active progressive MS with new clinical signs, use G35.B1 or G35.C1 depending on whether it is primary or secondary progressive.
Q: What was the old ICD-9 code for multiple sclerosis?
A: The multiple sclerosis ICD-9 code was 340. It mapped to G35 when the U.S. transitioned to ICD-10 in 2015.
Q: What is the difference between G35.B1 and G35.B2?
A: G35.B1 is active primary progressive MS, meaning there is current disease activity such as new MRI lesions or clinical signs. G35.B2 is non-active primary progressive MS, where the disease is present but currently stable with no new signs of activity.
Q: Can I use G35.D if the physician does not document the MS subtype?
A: You can use G35.D when the type is genuinely unknown or undocumented, but best practice is to query the provider first. Overusing G35.D without a query effort can attract payer scrutiny.
Q: Do I need to code MS-related symptoms separately?
A: Yes. Symptoms such as fatigue (R53.83), bladder dysfunction, depression, or optic neuritis that are documented and clinically managed at the encounter should be coded separately as additional diagnoses alongside the primary MS code.
Q: How does the 2026 MS coding change affect risk adjustment?
A: More specific coding allows payers and CMS to more accurately capture the severity and disease trajectory of each MS patient. Active progressive MS, for example, reflects a higher complexity patient than non-active unspecified MS, and the reimbursement and risk scores should reflect that.
Final Takeaway
The 2026 ICD-10 code for multiple sclerosis update is not just a minor administrative change. It represents a real shift in how the healthcare system documents, tracks, and reimburses for one of the most complex neurological conditions in medicine. Coders, billers, neurologists, and documentation specialists all need to be aligned on these new requirements.
The key things to remember: G35 alone does not fly anymore. Know your MS subtypes. Capture the activity status. Query your providers. And make sure your EHR and billing systems are updated.
Get this right, and you protect your revenue cycle. Get it wrong, and you are looking at a wave of rejections that will cost you time, money, and patient satisfaction.
This article is written for educational and informational purposes for healthcare professionals, medical coders, and billing specialists. Always refer to the official CMS ICD-10-CM guidelines for the most current coding rules.




