

Why M54.17 Is One of the Most Critical Spine Codes in 2026
Lower back pain is the number one cause of disability worldwide. A huge chunk of those cases involve nerve root compression that shoots pain straight down the leg. When that clinical picture shows up in the exam room, coders and providers reach for one code more than almost any other: M54.17 ICD-10 code.
M54.17 is the ICD-10 code for radiculopathy of the lumbosacral region. If you bill for spine-related services across orthopedics, neurology, pain management, physical therapy, or primary care, you will use this code constantly. The 2026 edition of ICD-10-CM keeps M54.17 active and billable through September 30, 2026, making it one of the most relevant musculoskeletal codes in use today.
Here is the problem — many providers and coders still mix up M54.17 with nearby codes like M54.16 (lumbar radiculopathy) or M54.50 (low back pain, unspecified). That confusion produces claim denials, payer audits, and lost reimbursement. In today’s tighter documentation environment, those mistakes cost more by the quarter.
So whether you are a coder cleaning up spine claims, a clinician documenting radiculopathy correctly, or a patient trying to understand that code on your paperwork — this guide covers everything, updated fully for 2026.
What Does M54.17 Mean? Breaking Down the Code
Before diving into symptoms and billing, start with the fundamentals. What exactly is the M54.17 diagnostic code?
M54.17 is an ICD-10-CM diagnosis code that officially describes Radiculopathy, Lumbosacral Region. It falls under Chapter 13 of ICD-10-CM, which covers Diseases of the Musculoskeletal System and Connective Tissue. More specifically, it sits within category M54 (Dorsalgia) and subcategory M54.1 (Radiculopathy).
Here is how the code breaks down character by character:
M = Musculoskeletal and connective tissue disease 54 = Dorsalgia (spinal pain) .1 = Radiculopathy (nerve root is compressed or irritated) 7 = Lumbosacral region (the junction of the lower lumbar spine and sacrum)
M54.17 literally translates to: a nerve root disorder located at the lumbosacral junction of the spine. That junction sits right around the L5-S1 vertebral level — one of the most load-bearing, movement-intensive spots in the entire human spine and, not coincidentally, one of the most common locations for disc herniation and nerve compression.
The term lumbosacral radiculopathy covers several related clinical descriptions providers may document. These include lumbar radiculitis, backache with radiating leg pain, and sciatic-type symptoms when no confirmed disc disorder has yet been identified. The ICD-10 radiculopathy lumbosacral code M54.17 captures all of these presentations under a single, specific, billable classification.
According to the 2026 ICD-10-CM guidelines, M54.17 is valid for all HIPAA-covered transactions from October 1, 2025 through September 30, 2026. Orthopedic practices use it most frequently, but providers across neurology, pain management, physical therapy, chiropractic care, and primary care bill it regularly.
Lumbosacral Radiculopathy Symptoms: What the Patient Actually Feels
Recognizing lumbosacral radiculopathy symptoms is the foundation of accurate diagnosis and correct code selection. When a patient walks into your office with classic nerve root compression from the lower back, the symptom picture is usually pretty distinct — once you know what to look for.
Pain That Travels Down the Leg
The defining feature of lumbosacral radiculopathy is radiating leg pain from lower back nerve compression. Unlike simple low back pain that stays localized, radiculopathy pain follows the path of the compressed nerve root. Patients often describe shooting, burning, or electric-type pain that starts in the lower back or buttock and travels down through the hip, thigh, calf, and sometimes all the way into the foot.
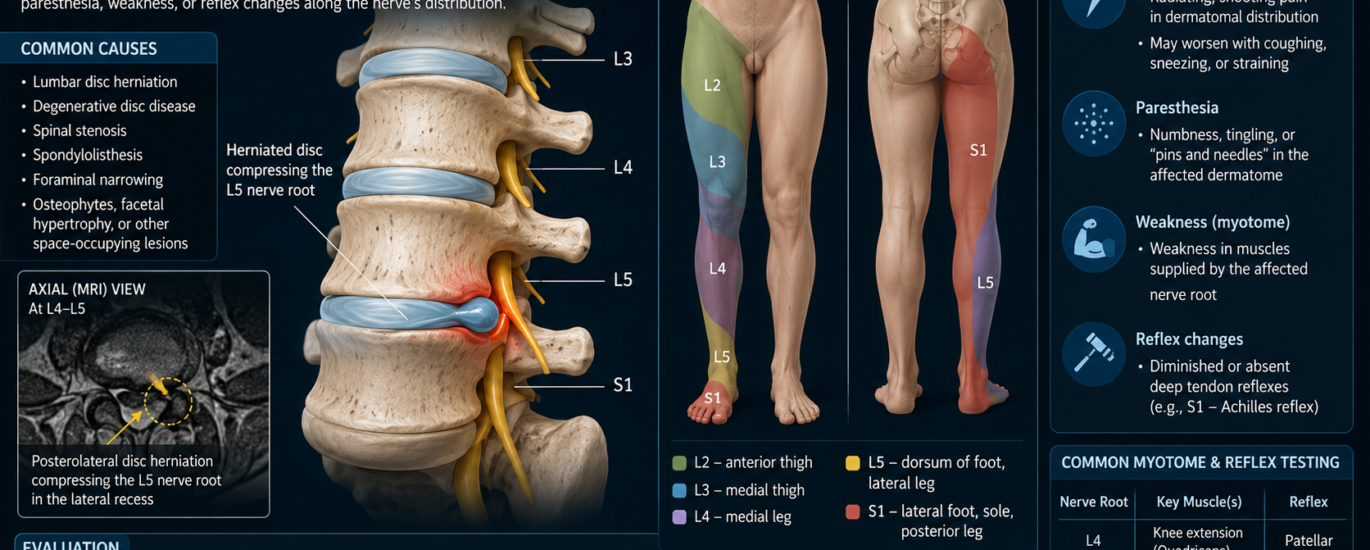
The specific pattern depends on which nerve root is affected. An L5 nerve root compression typically causes pain along the outer thigh and into the top of the foot. An S1 nerve root problem usually sends pain down the back of the thigh, through the calf, and into the heel or outer edge of the foot.
Numbness and Tingling
Along with the pain, most patients report a pins-and-needles sensation — sometimes described as the leg “falling asleep” — in the same dermatomal distribution as the pain. This numbness and tingling reflects sensory nerve fiber involvement. It is a strong clinical signal that true radiculopathy, rather than simple muscle pain, is present.
Muscle Weakness
In more significant nerve root compression cases, patients notice weakness in specific muscle groups. An L4 or L5 lesion may cause difficulty dorsiflexing the foot (known as foot drop in severe cases). An S1 lesion often produces weakness in plantarflexion — the patient may struggle to stand on their toes on the affected side.
Reflex Changes
On physical exam, clinicians typically find diminished or absent deep tendon reflexes on the affected side. A reduced knee jerk suggests L4 involvement. A reduced or absent ankle jerk is a classic sign of S1 radiculopathy. These objective exam findings are critical for documentation because they give coders the clinical support needed to justify M54.17 on any claim or audit.
Positive Straight Leg Raise
The Straight Leg Raise (SLR) test is one of the most reliable physical exam findings for lumbosacral radiculopathy. A positive result — reproducing radiating leg symptoms when the clinician raises the leg to 30-70 degrees with the patient supine — strongly suggests nerve root irritation and supports the use of M54.17 over a simpler pain code. The Bragard’s sign, where dorsiflexing the foot during the SLR increases symptoms, adds further diagnostic specificity.
Causes of Lumbosacral Radiculopathy
Understanding what drives nerve root compression lower back presentations helps providers document with the specificity that 2026 payers demand.
Disc Herniation
Disc herniation is the most common cause, particularly at the L4-L5 and L5-S1 levels. When the nucleus pulposus pushes through the annulus fibrosus and contacts a nerve root, it triggers both mechanical compression and a chemical inflammatory response that produces the classic radicular symptom pattern.
Foraminal Stenosis
Foraminal stenosis is another frequent culprit. The neural foramina — the openings through which nerve roots exit the spinal canal — naturally narrow with age as discs lose height and osteophytes (bone spurs) form. When a foramen narrows enough to compress the exiting nerve root, lumbosacral radiculopathy follows.
Degenerative Disc Disease
Degenerative disc disease at the lumbosacral junction accelerates foraminal narrowing and can trigger radiculopathy even without acute disc herniation. Age-related dehydration of the L5-S1 disc, combined with mechanical stress from the lordotic curve of the lumbar spine, makes this level particularly vulnerable.
Spondylolisthesis
Spondylolisthesis — where one vertebra slips forward over the one below it — can directly compress the nerve roots at the lumbosacral level. When imaging confirms vertebral slippage as the pain generator, coders should consider whether a more specific structural code (like M43.17) better captures the diagnosis.
Spinal Stenosis
Spinal stenosis of the lumbar or lumbosacral canal also produces radiculopathy-type symptoms, although the presentation often includes neurogenic claudication. Patients experience worsening pain and weakness with walking that improves with sitting or leaning forward.
M54.17 Billing Code CPT: How to Bill Accurately in 2026
Getting the M54.17 billing code CPT pairing right keeps claims clean, reduces payer pushback, and protects your revenue cycle. Here is a thorough breakdown of how to approach it.
CPT Codes Commonly Paired With M54.17
The following CPT codes regularly associate with treatment and evaluation of lumbosacral radiculopathy. Each can support M54.17 as the primary diagnosis when documentation justifies it.
Office Visit and Evaluation
CPT 99202-99215 covers new and established patient office visits, with the appropriate level determined by medical decision-making complexity or total time. Radiculopathy cases commonly justify moderate to high MDM levels because they involve a new or worsening presenting problem with multiple potential management options.
Imaging Services
CPT 72148 covers MRI of the lumbar spine without contrast — one of the most frequently ordered studies for confirmed or suspected lumbosacral radiculopathy. CPT 72100 covers lumbar spine X-rays when initial evaluation warrants them.
Electrodiagnostic Studies
CPT 95886 covers needle electromyography (EMG) of extremity muscles, which helps confirm nerve root involvement and determine the level of compression. CPT 95909 and related codes cover nerve conduction studies (NCS) that characterize the type and severity of nerve damage. These studies carry particular value when objective confirmation is needed before payers authorize interventional procedures.
Injections and Interventional Pain Management
CPT 62322 covers a lumbar or sacral interlaminar epidural steroid injection without imaging guidance. CPT 62323 covers the same procedure with fluoroscopic or CT guidance — the more common and payer-preferred approach. Providers frequently use these injections as first-line interventional treatment for radiculopathy lumbosacral region when conservative care has not resolved symptoms.
CPT 64483 covers transforaminal epidural steroid injection at the lumbar or sacral level. This approach more precisely targets the affected nerve root and is often preferred when imaging confirms a specific level.
Physical Therapy
CPT 97110 covers therapeutic exercises, which form the backbone of conservative treatment for lumbosacral radiculopathy. CPT 97012 covers traction — a frequently used manual therapy technique for nerve root decompression. CPT 97014 covers electrical stimulation, which can help manage radicular pain during the rehabilitation phase.
Trigger Point Injections
CPT 20552 covers injection into one or two muscle trigger points. CPT 20553 covers three or more trigger points. These apply when associated myofascial pain is documented alongside the radiculopathy.
Billing Tips That Actually Matter
Always document medical necessity before billing high-cost services. Before submitting for epidural injections or advanced imaging, your documentation must show the conservative treatment history — typically a trial of physical therapy, NSAIDs, and activity modification over four to six weeks — that justifies escalation. Payers, especially Medicare Advantage plans, aggressively audit spine injection claims in 2026 without documented prior conservative care.
Do not include the decimal point in electronic submissions. When filing claims electronically, submit the code as M5417, not M54.17. Some clearinghouses strip the decimal automatically, but others do not — and an incorrectly formatted code can trigger a rejection before the claim reaches the payer.
Add G89.29 for chronic radiculopathy. If the patient’s lumbosacral radiculopathy has persisted for 12 weeks or more, add G89.29 (Other Chronic Pain) as a secondary diagnosis code. This flags the condition as chronic to the payer, which supports authorization for ongoing physical therapy and repeated visits. Make sure the provider documents specific symptom duration in the chart — vague language like “longstanding” will not satisfy an auditor.
Note that laterality is not built into M54.17. The code itself does not differentiate between left-sided and right-sided radiculopathy. Clinical documentation absolutely should specify the side, however. Some payers require it for certain procedure authorizations, particularly for transforaminal injections where laterality determines which nerve root gets treated.
Lumbar Radiculitis vs Radiculopathy: Clearing Up the Confusion
Providers and coders frequently bump into this terminology issue, so it is worth addressing directly.
Lumbar radiculitis refers specifically to inflammation of a nerve root — the “-itis” suffix signals an inflammatory process. Radiculopathy is a broader term that covers any dysfunction of a nerve root, whether from inflammation, mechanical compression, ischemia, or any combination of those factors.
In the ICD-10-CM coding world, this distinction barely matters practically. M54.17 includes both radiculitis and radiculopathy of the lumbosacral region as accepted synonyms. When a provider documents “lumbosacral radiculitis,” the correct code is still M54.17. Clinicians often use the two terms interchangeably, and the code captures both.
The more important distinction for coding purposes is separating M54.17 from M54.16.
M54.16 vs M54.17: The Regional Difference
M54.16 covers radiculopathy specifically at the lumbar region (roughly L1 through L4). M54.17 specifically targets the lumbosacral junction, which refers to the L5-S1 level. If imaging and clinical findings show radiculopathy at both lumbar and lumbosacral levels — for example, L4, L5, and S1 nerve root involvement — some coders appropriately report both M54.16 and M54.17 on the same claim, since different spinal regions are involved. Always verify with your payer before doing so.
Lumbosacral Radiculopathy Exercises: What Treatment Actually Looks Like
Treatment directly shapes documentation, and documentation shapes billing. Understanding what lumbosacral radiculopathy exercises and conservative management actually look like gives coders and providers a shared language for claim support.
Physical Therapy Exercises
Physical therapy is the cornerstone of conservative treatment. Programs typically start with gentle neural mobilization exercises — movements designed to reduce nerve root sensitivity and improve mobility along the sciatic nerve pathway. McKenzie method exercises, which use repeated end-range lumbar movements to centralize and reduce radicular pain, carry strong evidence support.
Core Stabilization and Stretching
Core stabilization training addresses the deep lumbar stabilizers — the multifidus and transverse abdominis — which, when strengthened, reduce mechanical stress on the lumbosacral disc and facet joints. These exercises do not load the spine axially, so therapists can safely introduce them early in the rehabilitation process.
Stretching programs targeting the piriformis, hamstrings, and hip flexors reduce mechanical tension on the sciatic nerve and the lumbosacral nerve roots. Patients commonly continue these stretches as home exercise programs between formal PT sessions.
Traction and Medication
Traction therapy (CPT 97012) decompresses the neural foramen and can create temporary relief from nerve root compression, particularly for disc herniation-related radiculopathy. Both manual traction performed by a physical therapist and mechanical traction applied by specialized equipment appear in treatment plans for this condition.
Alongside exercise, NSAIDs and oral corticosteroids often serve as short-term pain management tools. Gabapentinoids like gabapentin or pregabalin target the neuropathic pain component of radiculopathy, and providers frequently document these as part of the non-surgical management plan. Muscle relaxants may be added when associated paraspinal muscle spasm is present.
Related ICD-10 Codes: Know When to Switch
Smart coding means knowing not only when to use M54.17, but also when a more specific code should take priority.
M51.17 — Intervertebral disc degeneration, lumbosacral region with radiculopathy. Use this code instead of M54.17 when imaging confirms a disc disorder as the direct cause of the radiculopathy. The disc code is more specific and supersedes M54.17 under the Excludes1 rules.
M54.16 — Radiculopathy, lumbar region. Use this code when nerve root compression is specifically at lumbar levels (L1-L4) rather than the lumbosacral junction.
M47.817 — Spondylosis, lumbosacral region, without myelopathy or radiculopathy. Use this when degenerative vertebral changes are present but no nerve root involvement is confirmed.
M54.40 through M54.42 — Lumbago with sciatica, unspecified/right/left. Use these codes when the clinical presentation includes both lower back pain and sciatica, and no structural cause has been identified. Note that M54.4x codes offer laterality options that M54.17 does not.
M43.17 — Spondylolisthesis, lumbosacral region. Use this when vertebral slippage is confirmed as the structural cause.
M48.062 — Spinal stenosis, lumbar region with neurogenic claudication. Use this when canal narrowing with neurogenic claudication is the primary finding.
S34.21XA — Injury of nerve root of lumbar spine, initial encounter. Use this for traumatic nerve root injuries rather than M54.17, which is reserved for non-traumatic radiculopathy.
Common Mistakes With M54.17 That Coders Make Every Single Day
Even certified coders and experienced billing teams fall into these traps. Knowing them ahead of time keeps your claims cleaner.
Using M54.17 When a Disc Code Applies
This is the most frequent and most costly mistake. When imaging confirms a herniated disc at L5-S1 causing nerve root compression, the right code is M51.17, not M54.17. The Excludes1 rules prohibit M54.17 from being used alongside intervertebral disc disorder codes from the M51 series at the same spinal region. Submitting both results in a denial.
Mixing Up M54.16 and M54.17
These two codes sit right next to each other in the ICD-10 hierarchy and look almost identical. The distinction is regional. M54.16 covers the lumbar spine (upper to mid-lumbar levels). M54.17 covers the lumbosacral junction (L5-S1). If the provider documents “L4-L5 radiculopathy,” you need M54.16. If they document “L5-S1 radiculopathy,” you need M54.17. When both levels are involved, you may need both codes — but verify payer policies before submitting them together.
Using M54.17 for Traumatic Injuries
M54.17 is specifically for non-traumatic lumbosacral radiculopathy. If the patient’s condition resulted from a fall, car accident, or other acute injury, the correct coding comes from the S34 series (spinal nerve injury codes). Using M54.17 for a trauma case is upcoding and will get flagged.
Submitting With Inadequate Documentation
Payers scrutinize radiculopathy claims more closely in 2026, particularly when the claim includes high-cost services like epidural injections or EMG studies. The chart must document the classic radiculopathy triad — radiating leg pain, objective neurological findings (reflex changes or sensory deficit), and a positive provocation test like the SLR. A note that simply says “back pain radiating to leg” is not enough.
Formatting the Code Incorrectly
When submitting electronically, use M5417, not M54.17. The decimal point can cause a claim format error in certain clearinghouse or payer systems.
Omitting Laterality From the Clinical Note
While M54.17 itself does not distinguish left from right, the clinical note should always specify the side affected. Certain associated CPT codes — like transforaminal epidural injections — require laterality documentation for accurate billing and prior authorization.
2026 Updates: What Changed and What to Watch This Year
The 2026 ICD-10-CM edition, effective October 1, 2025, keeps M54.17 intact as a valid, billable code with no changes to its description, hierarchy, or Excludes1 relationships. However, the broader coding environment around spine diagnoses has shifted considerably.
Tighter Payer Documentation Requirements
Multiple commercial payers and Medicare Advantage plans updated their Local Coverage Determinations (LCDs) going into 2026, raising the bar on what documentation must support before approving epidural steroid injections, nerve studies, and advanced imaging for radiculopathy diagnoses. Notes must now explicitly state the specific nerve root level, the clinical findings supporting radiculopathy, the failure of prior conservative treatment, and the functional impact on the patient’s daily activities.
AI-Assisted Documentation Is Now Mainstream
Many practices use ambient AI scribing platforms to generate SOAP notes. These tools are fast, but they do not always capture the granular exam findings that coders need for M54.17 claim support. Billing teams should audit AI-generated notes for radiculopathy cases to ensure objective findings — reflex changes, SLR result, dermatomal sensory loss, muscle weakness — appear explicitly in the assessment section, not just implied by the diagnosis line.
Telehealth Remains a Valid Care Channel
In 2026, telehealth coverage rules remain in effect for musculoskeletal complaints in most states. A telehealth note for lumbosacral radiculopathy must still contain the same specificity as an in-person note. A telehealth visit that lacks objective exam findings will struggle to support M54.17 on claims for associated imaging or injection procedures.
Physical Therapy Authorization Faces Increased Scrutiny
Many payers now require documented evidence of measurable functional improvement at 4 to 6 week intervals to continue authorizing physical therapy for radiculopathy. Coders and therapy teams need to ensure progress notes are specific enough to capture the functional gains that justify continuation of care.
FAQ:
What is the M54.17 ICD-10 code?
M54.17 is the ICD-10-CM diagnosis code for radiculopathy of the lumbosacral region. It describes compression or irritation of a nerve root at the lumbosacral junction (primarily the L5-S1 level), causing radiating pain, numbness, tingling, or weakness into the lower extremity.
What are the most common lumbosacral radiculopathy symptoms?
The most common symptoms include shooting or burning pain that travels from the lower back or buttock down through the leg, numbness and tingling in the leg or foot following a dermatomal pattern, muscle weakness in the foot or ankle, reduced deep tendon reflexes, and a positive Straight Leg Raise test.
What is the difference between M54.16 and M54.17?
M54.16 covers radiculopathy at the lumbar region (upper lumbar levels, roughly L1-L4). M54.17 covers the lumbosacral region, specifically the junction between the lumbar spine and sacrum at L5-S1. When both levels are affected, some coders report both codes, but payer policies vary on this.
What CPT codes pair with M54.17?
Commonly paired CPT codes include 99202-99215 for office visits, 72148 for lumbar MRI, 95886 for EMG, 62322/62323 for epidural steroid injections, 64483 for transforaminal injections, and 97110/97012 for physical therapy.
Can M54.17 and M51.17 be billed together?
No. These codes are mutually exclusive under the Excludes1 rules. When a lumbosacral disc disorder is confirmed as the cause of the radiculopathy, the more specific disc code (M51.17) replaces M54.17 — it does not supplement it.
Is M54.17 valid for traumatic nerve root injury?
No. M54.17 is for non-traumatic lumbosacral radiculopathy. Trauma-related nerve root injuries belong to the S34 code series.
What exercises help with lumbosacral radiculopathy?
The most effective exercises include McKenzie method extension and flexion movements, neural mobilization techniques, core stabilization exercises (bird-dog, dead bug), piriformis and hamstring stretching, and progressive lumbar stabilization progressions. A physical therapist should guide the exercise program based on the patient’s specific nerve root level and symptom behavior.
Does M54.17 require imaging to support the diagnosis?
Imaging is not strictly required for the diagnosis code itself, but payers expect imaging documentation before authorizing interventional procedures like epidural steroid injections. An MRI of the lumbar spine is the gold-standard study for confirming disc herniation or foraminal stenosis at the lumbosacral level.
Closing Thoughts:
M54.17 is one of the most clinically meaningful and financially significant codes in the entire spine billing world. It tells a complete patient story — nerve root compression at the lumbosacral junction, causing radiating leg pain from lower back nerve irritation, with real functional consequences for the patient’s daily life.
Getting this code right in 2026 means understanding the anatomy, knowing the Excludes1 rules cold, documenting the radiculopathy triad on every single visit note, and pairing the right CPT codes to the right clinical services. Providers who document with specificity and coders who know when M54.17 applies versus when M51.17 or M54.16 is the better choice — those are the teams that see clean claims, fast reimbursements, and fewer audit headaches.
The difference between a clean M54.17 claim and a denied one almost always comes down to documentation quality. So document the nerve level. Document the side. Document the exam findings. Document the failed conservative care. Do all of that, and M54.17 will work exactly the way it should — telling the payer precisely what the patient has and why they need the care you are providing.
This article reflects 2026 ICD-10-CM guidelines effective October 1, 2025. All coding guidance is for educational purposes. Always verify payer-specific policies and consult your compliance team for complex billing scenarios.pliance team for complex billing scenarios.




