

What Is M54.51 and Why Does It Matter in 2026?
If you are a medical coder, a billing specialist, or even a patient trying to decode your diagnosis paperwork, chances are you have stumbled across M54.51 vertebrogenic lower back pain and felt confused. You are not alone. This code gets misused, under-coded, and flat-out ignored more often than it should be.
So let’s break it all down in plain, simple language.
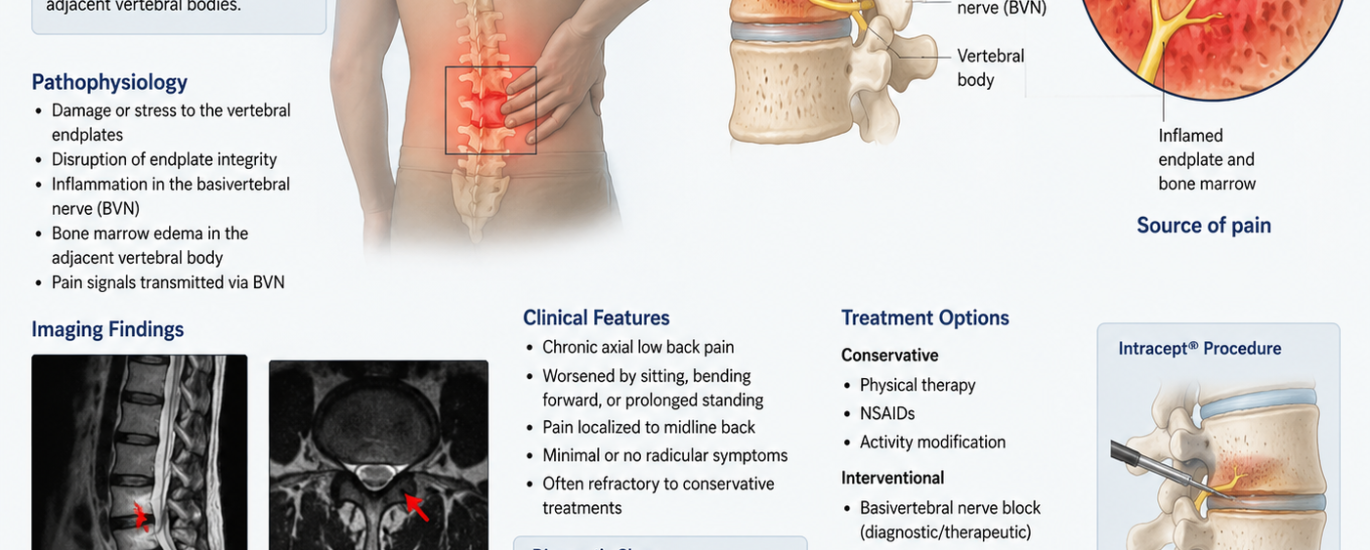
M54.51 is the ICD-10-CM diagnosis code specifically used to classify vertebrogenic low back pain — a type of chronic lower back pain that comes directly from the vertebral endplates and the surrounding bone marrow. Think of it this way: your spine has small, flat surfaces between the discs and the bones called endplates. When those endplates get damaged or inflamed, they send out constant pain signals through a tiny nerve called the basivertebral nerve. That is exactly what vertebrogenic pain is — and that is what M54.51 captures.
The 2026 edition of ICD-10-CM confirms that M54.51 became effective on October 1, 2025, making it active for all claims filed through September 30, 2026. This code is fully billable and specific, which means it is suitable for reimbursement purposes when the documentation supports it.
When Was ICD-10 Code M54.51 Introduced?
This is one of the most frequently searched questions about this code, so let’s answer it clearly.
ICD-10 code M54.51 was introduced on October 1, 2021. Before that date, providers were using the old umbrella code M54.5 — which simply said “low back pain” without specifying anything further. The Centers for Medicare and Medicaid Services (CMS), along with the National Center for Health Statistics (NCHS), realized that grouping all low back pain under one code was too vague. So they retired M54.5 and split it into three more precise codes:
- M54.50 — Low back pain, unspecified
- M54.51 — Vertebrogenic low back pain
- M54.59 — Other low back pain
This change allowed providers and coders to document and bill with much greater clinical accuracy. However, as of 2026, many practices are still using the old M54.5 without the fifth digit. That code has been invalid for over four years. If your EHR or superbill still shows M54.5 without the qualifier, it absolutely needs to be updated right now.
Understanding the Meaning of Vertebrogenic Low Back Pain
Before you can correctly assign the M54.51 diagnosis code, you need to understand what “vertebrogenic” actually means clinically.
The word comes from vertebra (the bones in your spine) and genic (originating from). So vertebrogenic low back pain literally means lower back pain that originates from the vertebra itself — specifically from the endplates, which are the thin cartilage-like surfaces at the top and bottom of each spinal bone.
Here is where it gets interesting. The vertebral endplates are heavily supplied by the basivertebral nerve (BVN). When those endplates break down due to disc degeneration, microfractures, or inflammatory changes, the BVN becomes hypersensitive. It starts firing chronic pain signals even when there is no new injury. This process creates a deep, persistent, axial pain that does not respond well to typical treatments like anti-inflammatories or physical therapy — because the source of the pain is inside the bone, not in the muscles or the disc itself.
This is fundamentally different from:
- Discogenic pain — which comes from the disc itself
- Radicular pain / sciatica — which travels down the leg following a nerve root
- Facet joint pain — which comes from the small joints at the back of the spine
- Myofascial pain — which comes from muscle tension
Vertebrogenic pain stays deep and central in the lower back. It does not shoot down into the legs in a dermatomal pattern, which is one of the key ways clinicians distinguish it from lumbar radiculopathy.
Symptoms of Vertebrogenic Low Back Pain
Recognizing the symptoms tied to the M54.51 diagnosis code is essential for providers who want to document accurately and for patients who want to understand what they are dealing with. Typically, vertebrogenic low back pain shows up in the following ways:
Deep, aching midline pain. The pain is usually centralized along the spine — not on one side or the other. It feels dull and heavy, almost like pressure from inside the bone.
Pain that gets worse with prolonged sitting or standing. Loading the spine for extended periods, especially in forward flexion, tends to flare up the symptoms significantly.
No significant leg pain or numbness. Unlike sciatica, vertebrogenic pain generally stays in the lower back. Radiating pain into the buttocks is possible but leg pain below the knee is not a typical feature.
Chronic, persistent nature. This type of back pain does not come and go. It tends to hang around for months or years, typically resisting conservative care.
Increased pain with loaded forward bending. Activities like picking something up off the floor or bending over a sink often aggravate the pain considerably.
Morning stiffness. Many patients wake up feeling stiff and achy, and this usually improves slightly after moving around — though it never fully resolves without targeted treatment.
What Causes Vertebrogenic Low Back Pain?
Several underlying factors can trigger the endplate damage and bone marrow changes that lead to vertebrogenic low back pain and ultimately justify the M54.51 diagnosis code.
Disc Degeneration
As intervertebral discs lose hydration and height over time, the mechanical stress on the adjacent endplates increases dramatically. The endplates were never designed to absorb that level of force alone, so they start to develop small stress fractures and structural damage.
Modic Changes on MRI
Modic changes are the MRI findings most closely associated with vertebrogenic low back pain. Named after Dr. Modic, these are changes in the bone marrow just above and below a degenerated disc, and they are classified into three types:
- Type 1 — Active inflammation and bone marrow edema. This is the type most strongly linked to ongoing, severe pain. On MRI, it appears dark on T1 and bright on T2 sequences.
- Type 2 — Fatty replacement of the bone marrow. This represents a more chronic, stable phase. Still very relevant for vertebrogenic pain.
- Type 3 — Sclerosis (bone hardening). Less commonly associated with active vertebrogenic pain.
When a patient’s MRI shows Type 1 or Type 2 Modic changes and the clinical presentation matches, the M54.51 code is almost always appropriate.
Aging and Wear-and-Tear
Simply put, the spine takes a beating over a lifetime. Heavy labor jobs, repetitive bending, poor posture, and cumulative loading all contribute to endplate breakdown over time.
Inflammatory and Autoimmune Processes
Emerging research from 2025 and 2026 also points to bacterial, inflammatory, and autoimmune factors as potential contributors to Modic changes and vertebrogenic pain. A 2026 literature review published in Skeletal Radiology confirmed that risk factors include mechanical disruption, inflammation, and autoimmune etiologies increasingly tied to nociceptive signaling from the basivertebral nerve.
Diagnosis: How Providers Confirm M54.51
Accurately diagnosing vertebrogenic low back pain requires more than just a clinical exam. Here is what providers typically look for before assigning the M54.51 diagnosis code:
MRI with Modic changes. Imaging evidence of Type 1 or Type 2 Modic changes on MRI is the gold standard for supporting a vertebrogenic diagnosis. The provider must clearly document this link in the clinical notes.
Clinical correlation. The patient’s symptoms must match the imaging findings. An MRI showing Modic changes on a patient whose pain is clearly radicular (shooting into the leg) would not support M54.51 on its own.
Ruling out other causes. Providers must confirm the pain is not better explained by disc displacement, facet joint disease, spinal stenosis, or piriformis syndrome before assigning this specific code.
Documentation specificity. The clinical note must use language like “vertebrogenic,” “endplate-related,” or “Modic change-associated low back pain” to support the code assignment. Vague documentation like “low back pain” defaults the coder to M54.50 instead.
M54.51 Billing Tips for 2026: What Every Coder Needs to Know
Getting your billing right with the M54.51 diagnosis code can mean the difference between clean claim approvals and frustrating denials. Here are the most important billing tips for FY2026:
Always Match Code Specificity to Documentation
M54.51 has the strictest documentation standards of the entire M54.5x group. You cannot assign this code just because the patient has back pain and happens to have an MRI. The provider note must explicitly tie the imaging findings to the pain source. If the documentation does not say “vertebrogenic” or reference endplate pathology, default to M54.50 and follow up with the provider for clarification.
Never Mix M54.51 with Redundant Codes
You cannot bill M54.51 alongside diagnoses that already explain the back pain. For example:
- Do not pair M54.51 with M51.360 (disc degeneration with discogenic back pain, lumbar region). These two codes have an Excludes1 relationship — meaning they cannot appear on the same claim.
- Do not pair M54.51 with M54.4x (lumbago with sciatica). Sciatica implies a nerve root cause, which directly conflicts with the vertebrogenic origin.
Add a Secondary Chronic Pain Code When Appropriate
When coding for chronic vertebrogenic low back pain, consider adding G89.29 (Other chronic pain) as a secondary diagnosis. This supports medical necessity, especially for procedures like basivertebral nerve ablation (Intracept procedure).
Stop Using the Old M54.5
Seriously, this one cannot be stressed enough. The parent code M54.5 has been invalid since October 1, 2021. Submitting claims with M54.5 in 2026 will result in immediate rejections. Always use M54.50, M54.51, or M54.59 with the fifth digit.
Verify Payer-Specific Rules
Some commercial payers and Medicare Administrative Contractors (MACs) have specific Local Coverage Determinations (LCDs) for basivertebral nerve ablation procedures tied to M54.51. Always check the LCD associated with the procedure code before submitting. Documentation requirements can vary between payers.
Related ICD-10 Codes You Should Know
When working with vertebrogenic low back pain, understanding the full coding landscape around M54.51 helps you code accurately and avoid conflicts:
| Code | Description |
|---|---|
| M54.50 | Low back pain, unspecified — use when documentation lacks clinical specificity |
| M54.59 | Other low back pain — use when specific context exists but it is not vertebrogenic |
| M54.41 / M54.42 | Lumbago with sciatica, right/left — for pain with confirmed sciatic nerve involvement |
| M51.16 / M51.17 | Intervertebral disc degeneration, lumbar — when disc degeneration is the primary documented source |
| M48.061 / M48.062 | Spinal stenosis, lumbar — for lumbar canal narrowing |
| G89.29 | Other chronic pain — useful secondary code for chronic vertebrogenic presentations |
| M54.16 | Lumbar radiculopathy — for nerve root irritation causing leg symptoms |
Common Mistakes Coders Make with M54.51
These errors show up constantly in billing audits, and they are completely avoidable:
Using M54.50 when M54.51 is clearly supported. This is technically under-coding. When imaging and documentation confirm a vertebrogenic source, defaulting to the unspecified code is inaccurate and can trigger post-payment audits.
Assigning M54.51 without imaging support. Flipping the other way — coding M54.51 just because the patient has chronic back pain — is over-coding. Always make sure Modic changes or endplate pathology appear on the MRI report and are documented by the provider.
Still submitting M54.5 (without the fifth digit). This is the most common and most preventable mistake in 2026. That code is dead. Use the subcategories.
Pairing M54.51 with conflicting structural codes. Billing M54.51 alongside discogenic pain codes or sciatica codes creates claim edits because of Excludes1 restrictions.
Ignoring documentation clarity. If the clinical note uses generic language like “lumbar pain” or “back ache,” the coder cannot assume a vertebrogenic cause. Coders need to query the provider rather than guessing.
2026 Updates: What Changed with M54.51 This Year
The FY2026 ICD-10-CM cycle (effective October 1, 2025) did not introduce changes to the code description or structure of M54.51 itself. The code definition remains stable. However, several important 2026 updates affect how this code is used in practice:
April 1, 2026 mid-year update. The mid-year ICD-10-CM update, which took effect April 1, 2026, introduced additional adjacent musculoskeletal codes. Coders should review updated crosswalk tables to ensure no new Excludes relationships affect M54.51 claims.
AI-assisted coding adoption. In 2026, more practices are deploying AI coding tools that automatically flag when M54.51 should be applied based on clinical notes and MRI reports. These tools are significantly reducing under-coding of vertebrogenic pain.
Expanded coverage for basivertebral nerve ablation. Several major payers have updated their LCDs in 2025-2026 to expand coverage for the Intracept procedure (basivertebral nerve ablation), which is directly tied to M54.51 as the supporting diagnosis. This makes accurate use of M54.51 more financially significant than ever.
Growing clinical recognition. A major 2026 literature review confirmed that vertebrogenic back pain is significantly underdiagnosed, with up to 80-90% of chronic low back pain patients receiving a nonspecific LBP diagnosis when a more specific one — including M54.51 — would be clinically appropriate. This makes proper documentation and coding a genuine patient care issue, not just a billing technicality.
Treatment Options for Vertebrogenic Low Back Pain
Understanding what treatment connects to the M54.51 code helps both clinicians and coders appreciate the full clinical picture.
Basivertebral nerve (BVN) ablation — also called the Intracept procedure — is currently the most targeted treatment for confirmed vertebrogenic low back pain. Using radiofrequency energy delivered through a small probe into the vertebra, the procedure quiets the overactive basivertebral nerve without damaging the spine’s structure. Multiple randomized controlled trials have confirmed its effectiveness for patients with Modic Type 1 or Type 2 changes who have not responded to conservative care.
Conservative care — including physical therapy focused on spine stabilization, anti-inflammatory medications, and activity modification — is typically the first-line approach. However, these methods often provide incomplete relief for true vertebrogenic pain because they do not address the internal nerve source.
Steroid injections — while commonly used for other types of back pain — generally show limited effectiveness for vertebrogenic pain, since the inflammation is inside the bone rather than in the epidural space.
Frequently Asked Questions (FAQ)
What is the ICD-10 code M54.51? M54.51 is the ICD-10-CM diagnosis code for vertebrogenic low back pain — chronic lower back pain caused by damaged or inflamed vertebral endplates, confirmed by MRI findings such as Modic changes.
When was ICD-10 code M54.51 introduced? M54.51 was introduced on October 1, 2021, when CMS and NCHS retired the old M54.5 code and replaced it with three more specific codes: M54.50, M54.51, and M54.59.
What is the difference between M54.5 and M54.51? M54.5 was a broad, unspecified code for all low back pain. It was retired in 2021. M54.51 is the specific successor code used only when vertebrogenic pathology is documented and supported by imaging.
Does M54.51 require imaging to code? Yes, in practice. While the ICD-10 manual does not technically mandate imaging as a coding requirement, the clinical standard is that MRI evidence of Modic changes or vertebral endplate abnormality is necessary to support the vertebrogenic diagnosis and justify M54.51.
Can I use M54.51 and M54.50 on the same claim? No. These codes describe two different levels of specificity for the same condition. You code either one or the other based on the documentation — never both together.
Is vertebrogenic low back pain the same as discogenic pain? No. Discogenic pain originates from the disc itself. Vertebrogenic pain originates from the vertebral endplates and the bone. Though they are related (disc degeneration often leads to endplate damage), they are distinct conditions with different codes and different treatment approaches.
What is the 2026 status of M54.51? M54.51 is fully active and billable in the 2026 ICD-10-CM cycle, effective from October 1, 2025 through September 30, 2026.
Final Takeaway
The M54.51 vertebrogenic lower back pain code is not just a billing formality — it represents a genuine shift in how medicine understands and treats one of the most common and disabling conditions in the world. Getting it right matters for patients who deserve targeted care, for providers who need clean claims, and for coders who want to stay audit-proof in 2026.
Always follow the documentation, match the code to the clinical evidence, and ditch the old M54.5 for good. The five minutes it takes to code correctly can save hours of rework — and, more importantly, it puts the right diagnosis on the right patient’s chart.




