

If you work in medical billing, coding, or you just got a diagnosis slip that says “M54.9” or “M54.89” and you have no idea what that means — you’re in the right place. A lot of people, including experienced coders, mix these two up every single day. And that mistake? It can cost your practice real money through denied claims and audit flags.
In this guide, we’re breaking down everything you need to know about m54.89 vs m54.9 in plain, no-fluff language. We’ll cover what each code means, how to tell them apart, what symptoms they represent, why providers use one over the other, and how to keep your billing clean in 2026. Whether you’re a coder, a clinician, a biller, or a patient trying to understand your diagnosis, this article has you covered.
What Is Diagnosis M54? Understanding the Parent Code First
Before we get into the comparison, let’s talk about where both codes live. M54 is the ICD-10-CM parent code for dorsalgia, which is basically the clinical term for back pain. It falls under Chapter 13 of the ICD-10-CM system, which covers Diseases of the Musculoskeletal System and Connective Tissue.
Here’s the thing — M54 by itself is NOT billable. It’s what we call a header code. You can’t throw M54 on a claim and expect it to go through. You need a more specific code underneath it, and that’s exactly where M54.9 and M54.89 come in.
The entire M54 family covers back and spine pain across multiple regions. Think of it as the umbrella, and M54.9 and M54.89 as two different spots under that umbrella — close to each other, but not the same.
What Is M54.9? The “Unspecified” Dorsalgia Code
So, what is M54.9 exactly? The official ICD-10-CM description is Dorsalgia, unspecified. In simpler terms, it means back pain — but the provider’s documentation doesn’t narrow it down any further.
The two official synonyms for M54.9 are:
- Backache NOS (Not Otherwise Specified)
- Back pain NOS
That little “NOS” tag is the key. It tells you — and the payer — that the provider wrote “back pain” but never specified where in the back, what’s causing it, or whether the patient has an acute or chronic situation. It’s essentially the coding equivalent of saying, “the patient has back pain, and that’s all we know right now.”
When someone asks what does diagnosis code m54 9 mean, the honest answer is: it means the patient has back pain that hasn’t been pinpointed any further. It’s valid, it’s billable, and it’s fully active in the FY2026 code set — but it should only be used when the documentation genuinely doesn’t support anything more specific.
When M54.9 Is Appropriate
M54.9 works in specific, legitimate situations. For example:
- A patient walks in for the first visit with vague, diffuse back pain. No imaging yet. No exam findings pointing to a clear location or cause.
- The provider documents “back pain” without indicating the region, onset characteristics, or contributing factors.
- A telehealth encounter where a full physical exam hasn’t happened yet.
In those cases, M54.9 is your code. Use it. But — and this is important — once you have more information, you must update the code.
What Is Diagnosis M54.89? The “Other Dorsalgia” Code
Now let’s talk about what is diagnosis m54.89. The official description is Other dorsalgia. This is where things get a little more nuanced, and honestly, where a lot of coders trip up.
M54.89 is the “catch-all” for dorsalgia presentations that are identifiable enough to be something other than completely unspecified — but they don’t fit neatly into any of the more specific M54 subcodes like M54.50 (low back pain), M54.51 (vertebrogenic low back pain), M54.2 (cervicalgia), or M54.3 (sciatica).
Think of it this way: M54.9 says “I don’t know where the pain is.” M54.89 says “I know it’s back-related pain, and I know it’s something, but it doesn’t fit the other boxes.”
Common clinical scenarios where M54.89 applies include:
- Chronic sacral pain lasting more than three months
- Back pain involving multiple regions without a dominant site
- Dorsalgia linked to systemic conditions where the exact spinal segment isn’t isolated
- Thoracic-lumbar junction pain that doesn’t map to a single code
- Post-procedural back pain that injury codes don’t cover
M54.89 is valid from October 1, 2025 through September 30, 2026 for all HIPAA-covered transactions. It’s actively used in Family Practice, Internal Medicine, and Orthopedics.
M54.89 vs M54.9: The Side-by-Side Comparison
Here’s the real difference between these two codes laid out clearly:
| Feature | M54.9 | M54.89 |
|---|---|---|
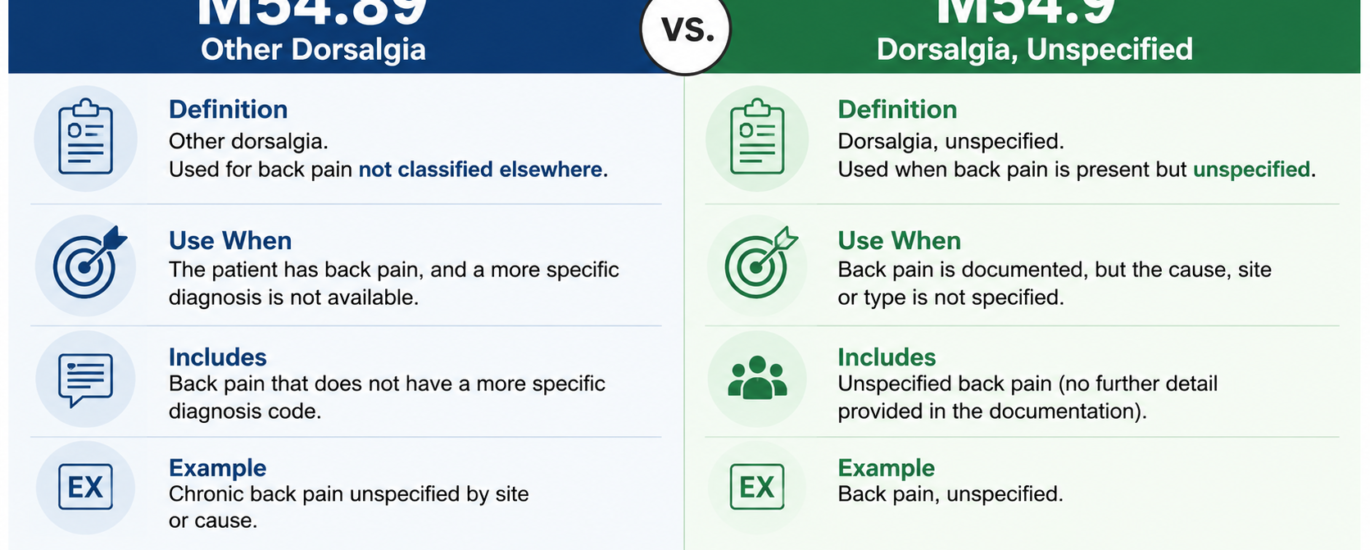
| Official Name | Dorsalgia, unspecified | Other dorsalgia |
| Specificity Level | Lowest (unspecified) | Medium (specified as “other”) |
| Documentation Needed | No location or cause documented | Location or type partially identified |
| Synonyms | Backache NOS, Back pain NOS | Chronic sacral pain, multi-region dorsalgia |
| Audit Risk | Higher if overused | Lower if documented properly |
| Best Used When | First-visit, vague, no exam data | Known type of back pain not in other codes |
| Payer Scrutiny | Higher scrutiny from commercial payers | Moderate scrutiny |
The core rule here is specificity. ICD-10-CM always pushes coders toward the most specific code the documentation supports. M54.9 sits lower on the specificity ladder than M54.89. So if your notes describe the type or region of pain — even partially — M54.89 typically gives you the better fit over M54.9.
Symptoms Associated With These Codes
Because both codes fall under dorsalgia, they share overlapping symptom profiles. However, the clinical picture is what drives the code selection.
Symptoms Common to M54.9 (Back Pain Unspecified)
- General aching or soreness across the back (no clear location)
- Stiffness that improves or worsens with movement
- Pain that the patient describes vaguely without pointing to a spot
- Discomfort that fluctuates without a pattern
- Fatigue-related back tension with no structural finding
Symptoms Common to M54.89 (Other Dorsalgia)
- Chronic sacral or low-thoracic pain lasting over three months
- Multi-region back pain where several areas hurt simultaneously
- Back pain with reduced range of motion and documented tenderness on palpation
- Post-procedural aching not attributed to a specific injury
- Dull, persistent pain with intermittent flare-ups and documented exam findings
If a provider documents “dull aching aggravated by movement with localized tenderness on exam,” that note supports M54.89 — not M54.9 — because there’s clinical detail beyond just “back pain.”
Causes and Risk Factors Behind M54 Dorsalgia
Understanding the causes helps coders match documentation to the right code. M54.89 vs M54.9 isn’t just a clerical choice — it reflects what the provider actually sees, documents, and communicates in the record.
Common Causes Documented Under M54.89
- Degenerative processes: Age-related wear on spinal structures, disc degeneration
- Biomechanical stress: Poor posture, repetitive occupational movements, heavy lifting
- Systemic inflammation: Conditions like ankylosing spondylitis affecting multiple spinal regions
- Obesity: Excess body weight increasing mechanical load on the spine
- Post-procedural changes: Residual pain following spinal surgery or injections
- Genetic predisposition: Family history of musculoskeletal conditions
Why M54.9 Gets Used (Even When It Shouldn’t)
Ironically, M54.9 often gets used not because the documentation is vague, but because the coder doesn’t take time to review the full note. That’s a compliance problem. Back pain is one of the most common diagnoses in the United States — affecting roughly 8 out of 10 people at some point in their lives — and because it’s so frequent, coding shortcuts are tempting. Resist them.
2026 Updates: What’s New for M54.89 and M54.9
Let’s talk about what changed (and what didn’t) heading into the 2026 fiscal year.
Both Codes Stay Active — No Changes This Cycle
Both M54.89 and M54.9 remain fully active in the FY2026 code set, covering October 1, 2025 through September 30, 2026. CMS did not delete, revise, or restructure either code this cycle. So if your workflow already uses them correctly, keep going — but read the updates below because the codes around them did shift.
The M54.5 Retirement Still Trips Up Coders
CMS retired the broad M54.5 code in a prior update, and the ripple effects still show up in billing queues today. That retirement forced coders to move to the more granular M54.5x family (M54.50, M54.51, M54.59). The problem? Many coders who used to default to M54.5 now default to M54.9 instead — and that’s wrong. When documentation identifies lumbar pain, M54.50 is the right code, not M54.9. The retirement changed the codes; it didn’t lower the documentation standard.
The M51.36x Expansion Creates New Excludes1 Traps
CMS introduced expanded sixth-character detail for lumbar and lumbosacral disc degeneration in FY2025, and those rules carry directly into 2026. Specifically, M51.360 (disc degeneration with discogenic back pain, lumbar region) now carries an Excludes1 relationship with M54.50. That means you cannot bill both codes on the same claim. Coders who haven’t updated their crosswalks hit this wall hard — and the denial comes fast.
Payers Are Using AI to Flag Unspecified Codes
In 2026, more commercial payers and Medicare Advantage plans now run AI-driven claim review tools that actively flag unspecified codes — including M54.9 — whenever clinical documentation suggests a more specific code was available. That’s not just a denial risk anymore. It triggers an audit flag that follows the claim through review. Stay ahead of it by reviewing the note before you assign the code.
Documentation Quality Now Drives Revenue
CMS and OIG continue to spotlight back pain coding as a high-risk area. Improper payments in the M54 dorsalgia category rack up billions of dollars in billing errors annually. If your practice defaults to M54.9 without reviewing the note, that habit now carries real financial and compliance consequences in 2026.
Billing Tips for M54.89 and M54.9 in 2026
After a decade of working with medical billing, here are the practical tips that actually move the needle:
Tip 1: Never use M54.9 as a default code. Review the provider’s note before assigning it. If the note contains any location indicator, exam finding, or clinical detail, you likely have enough to use something more specific — like M54.89 or a regional code.
Tip 2: Upgrade codes when new information arrives. If you coded M54.9 on visit one, and visit two includes imaging results or an exam that identifies the pain region, update the code. Failing to do so is one of the fastest ways to invite payer scrutiny.
Tip 3: Document acuity clearly. Acute, subacute, and chronic presentations all affect code selection and justification. M54.89 works for chronic sacral pain, for example — but “chronic” needs to be in the documentation. Don’t code chronicity if the provider didn’t document it.
Tip 4: Verify payer-specific policies. Some commercial payers have Local Coverage Determinations (LCDs) that restrict unspecified codes. Before submitting M54.9, run it against the payer policy.
Tip 5: Link your ICD-10 to the correct CPT. On the superbill, make sure the diagnosis code connects logically to the procedure code. An M54.9 tied to an MRI of the lumbar spine will likely draw scrutiny because an unspecified back pain code rarely justifies advanced imaging on its own. M54.89 with a documented multi-region presentation gives you stronger medical necessity footing.
Tip 6: Use secondary codes where appropriate. For chronic pain documentation, you can pair M54.89 with G89.29 (Other chronic pain) as a secondary code to strengthen the claim.
Related Codes You Should Know
Understanding the broader M54 family makes you a better coder. Here’s a quick reference for codes that interact with M54.89 and M54.9:
- M54.50 — Low back pain, unspecified (lumbar region, no specific cause)
- M54.51 — Vertebrogenic low back pain (requires imaging or clinical confirmation)
- M54.59 — Other low back pain (mechanical, characterized lumbar pain)
- M54.2 — Cervicalgia (neck pain)
- M54.3 — Sciatica
- M54.4 — Lumbago with sciatica
- M54.6 — Pain in thoracic spine
- G89.29 — Other chronic pain (secondary code for chronic dorsalgia)
- M51.360 — Lumbar disc degeneration with discogenic back pain (Excludes1 with M54.50)
Knowing these related codes prevents upcoding, downcoding, and Excludes1 violations that trigger denials.
Common Mistakes Coders Make With M54.89 vs M54.9
These are the real-world errors that show up in audits and denial queues every week:
Mistake 1: Using M54.9 when the note supports a regional code. The most frequent error. A note says “lumbar back pain” and the coder assigns M54.9. The correct code is M54.50. This is a specificity failure.
Mistake 2: Using M54.89 without documentation of what “other” means. M54.89 needs clinical substance behind it. If the note just says “back pain” with no detail, M54.89 is no more defensible than M54.9 — and it may look like upcoding.
Mistake 3: Not updating codes across visits. M54.9 on the first visit is fine. Keeping M54.9 on visit five when imaging results have arrived is not.
Mistake 4: Billing M54.50 and M51.360 together. These codes have an Excludes1 relationship. Using both on the same claim will get denied.
Mistake 5: Ignoring payer LCDs. Some Medicare Administrative Contractors have policies that restrict or require additional documentation for unspecified back pain codes. Skipping this review is a costly habit.
Mistake 6: Assuming M54.89 is more specific just because it has more digits. Both M54.9 and M54.89 are five-character codes. “More specific” in ICD-10 doesn’t mean more digits — it means more clinical detail is captured. M54.89 is only more appropriate when the documentation actually describes an identifiable type of dorsalgia that doesn’t fit elsewhere.
Frequently Asked Questions (FAQ)
What does diagnosis code M54.9 mean? M54.9 is the ICD-10-CM code for Dorsalgia, unspecified. It means the patient has back pain, but the clinical documentation doesn’t give enough detail to identify the region, cause, or type. Providers and coders also call it Backache NOS or Back Pain NOS.
What is M54.89 used for? M54.89 is used for Other dorsalgia — back pain presentations that are identifiable as something other than completely unspecified, but don’t fit any of the more specific M54 subcodes. Common examples include chronic sacral pain lasting over three months and multi-region dorsalgia with documented exam findings.
What is the real difference between M54.89 vs M54.9? The key difference is the level of clinical specificity in the documentation. M54.9 applies when the provider documents only that the patient has back pain, with no further detail. M54.89 applies when there’s some clinical detail — a partial location, a type, or characteristics — but the pain still doesn’t fit a more precise regional code. M54.89 sits one step above M54.9 on the specificity ladder.
Can I use M54.9 and M54.89 together on the same claim? No. These codes are mutually exclusive. You pick one based on what the documentation supports for that encounter.
Is M54.9 still valid in 2026? Yes. M54.9 is fully active in the FY2026 ICD-10-CM code set, effective October 1, 2025 through September 30, 2026, with no modifications.
Is M54.89 active for 2026? Yes. M54.89 is also confirmed active for FY2026 with no changes. It became effective on October 1, 2025 for the current fiscal year.
When should I use M54.9 vs M54.50? Use M54.50 when the provider specifically documents lumbar or low back pain. Use M54.9 only when the back pain is genuinely unspecified with no regional indicator in the documentation.
What specialty uses M54.89 most often? M54.89 is frequently used in Family Practice, Internal Medicine, and Orthopedics, especially for patients with complex back presentations that cross multiple regions or involve chronic sacral conditions.
Can a patient self-diagnose M54.9 or M54.89? No. These are provider-assigned diagnostic codes. A patient describes their pain to a doctor, but the treating provider assigns the ICD-10 code, and a trained coder translates it into the final diagnosis based on the clinical documentation.
Does M54.89 require imaging to bill? Not always, but your documentation must support medical necessity. If imaging exists and confirms a structural finding, select the code that reflects that finding as specifically as possible. M54.89 without supporting clinical notes opens the door to challenges from payers.
Final Thoughts: Pick the Code the Documentation Earns
Here’s the bottom line after everything we’ve walked through: the documentation tells you the code, not the other way around. That’s the most important lesson any coder can carry.
M54.9 isn’t a bad code. It’s a necessary one for genuinely unspecified back pain presentations. But it gets abused when coders use it as a shortcut, and in 2026 — with payers using smarter claim review tools — that shortcut is getting more expensive.
M54.89 is your friend when the clinical picture is clearer but still doesn’t fit a specific regional code. Use it confidently when the documentation backs you up. Document acuity. Capture the region. Note the laterality if available. And always, always update the code when new clinical information arrives.
Back pain is one of the most commonly coded conditions in American healthcare. Getting the m54.89 vs m54.9 distinction right isn’t just about compliance — it’s about being a professional who represents patients and providers accurately, every single time.




