If you work in medical billing, coding, or clinical documentation, there is one code you will run into over and over again: I48.91 — the ICD 10 code for AFib unspecified. This single code carries a lot of weight. Get it right and claims sail through. Get it wrong and you are staring at denials, audit flags, and lost revenue.
This guide breaks everything down clearly so that coders, clinicians, and billing teams can walk away with the full picture. We are talking about what AFib is, why the “unspecified” label matters, how billing actually works, what mistakes people keep making in 2026, and what has changed in the latest ICD-10-CM update cycle.
Let’s get into it.
What Is Atrial Fibrillation? (And Why the Code Matters So Much)
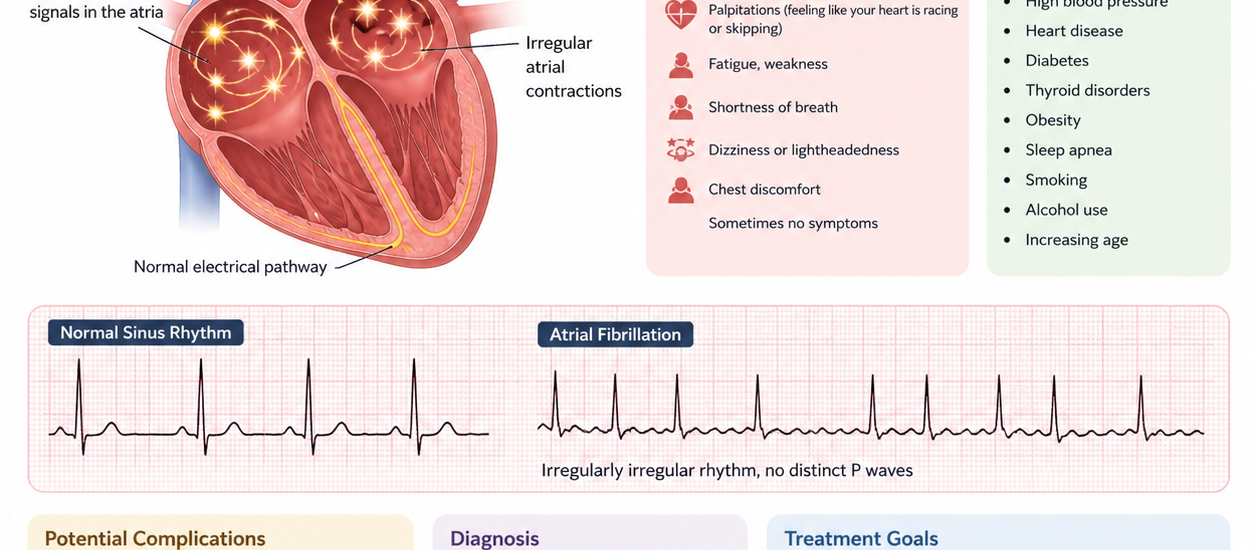
Atrial fibrillation, commonly called AFib or AF, is the most common heart rhythm disorder in the United States. It happens when the upper chambers of the heart, called the atria, fire electrical signals in a chaotic, disorganized way instead of beating in a steady, coordinated rhythm. Because of this, the lower chambers cannot pump blood efficiently.
The result? An irregular, often rapid heartbeat that increases the risk of stroke, blood clots, heart failure, and other serious complications. AFib affects millions of Americans, and that number keeps climbing every year as the population ages.
From a medical coding standpoint, atrial fibrillation falls under the I48 category in the ICD-10-CM classification system. This category covers both atrial fibrillation and atrial flutter. Within that category, the type of AFib you document determines the exact code you use, and using the wrong one is a billing landmine.
What Does “Unspecified” Actually Mean in Atrial Fibrillation ICD 10?
Here is the deal with “unspecified.” When a provider diagnoses a patient with AFib but does not document the specific type, whether it is paroxysmal, persistent, longstanding persistent, or permanent, the coder defaults to I48.91.
This does not mean the patient has some mysterious or unclear condition. It simply means the clinical notes did not include enough detail to assign a more specific code. Maybe the provider wrote “AFib” and left it at that. Maybe the patient is newly diagnosed and the type has not been confirmed yet. Either way, I48.91 steps in as the appropriate code when specificity is missing.
I48.91 — Unspecified Atrial Fibrillation is a fully billable, specific ICD-10-CM diagnosis code. It has been valid and active every year from 2016 through the 2026 edition.
Symptoms of Atrial Fibrillation You Should Know
Understanding the clinical picture helps coders spot documentation gaps and ask the right questions. Patients with AFib typically show up with the following symptoms:
Palpitations are the most reported complaint. Patients describe their heart as fluttering, racing, flopping, or just beating “wrong.” This is often what sends them to the ED in the first place.
Shortness of breath is extremely common, especially with exertion or when lying flat. When the heart is not pumping efficiently, the lungs can feel it.
Fatigue hits hard because the body is not getting well-oxygenated blood in the normal steady supply. Patients often say they feel wiped out doing normal activities.
Dizziness or lightheadedness can come on suddenly, particularly if the heart rate is very fast. This is especially relevant in AFib with RVR (rapid ventricular response) cases.
Chest discomfort or pressure can accompany AFib, though this may also signal a co-occurring condition like coronary artery disease.
Reduced exercise tolerance is a big quality-of-life issue. Many patients notice they cannot walk as far or climb stairs as easily as before.
Importantly, some patients have no symptoms at all. AFib gets picked up on a routine EKG or during a workup for something else entirely. These asymptomatic patients still need proper coding.
Causes and Risk Factors for AFib
AFib does not appear out of nowhere. Several underlying conditions and lifestyle factors drive it. Knowing the causes helps with secondary coding, which can actually improve reimbursement accuracy.
High blood pressure (hypertension) is the single most common driver. It puts constant stress on the heart walls and eventually triggers electrical remodeling.
Coronary artery disease disrupts blood flow to the heart muscle, creating the perfect environment for abnormal electrical signals.
Heart valve disease, especially mitral valve problems, is strongly linked to AFib. The left atrium stretches and the risk climbs.
Obesity raises the risk significantly. Fat tissue around the heart releases inflammatory signals that can trigger arrhythmia.
Obstructive sleep apnea is a major and often under-coded contributing factor. When oxygen levels drop repeatedly during sleep, the heart electrical system takes a hit.
Diabetes and chronic kidney disease both create systemic stress that wears down cardiac function over time.
Thyroid disorders, particularly hyperthyroidism, are a classic cause that every coder should watch for in the medical record.
Alcohol use, heavy or even moderate in some people, can trigger AFib episodes. The term “holiday heart” came from exactly this phenomenon.
Aging remains a primary risk factor. The risk of developing AFib jumps significantly after age 65 and continues to rise with each decade.
Recent cardiac surgery is another trigger. AFib in the post-operative period is extremely common and requires careful documentation for accurate coding.
The Full ICD 10 AFib Code Family: Know Your Options
Understanding I48.91 means understanding the whole I48 family. Here is the complete current picture for 2026:
I48.0 — Paroxysmal Atrial Fibrillation (PAF ICD 10) This is the code for AFib that comes and goes on its own, typically lasting less than 7 days. This is what most people mean when they say PAF ICD 10. Episodes self-terminate, though some need cardioversion.
I48.11 — Longstanding Persistent Atrial Fibrillation Used when AFib has been ongoing for more than 7 days, generally more than 12 months, and requires intervention to stop.
I48.19 — Other Persistent Atrial Fibrillation This catches persistent AFib that is documented as “chronic persistent” or when it does not fit neatly into the longstanding category.
I48.20 — Chronic Atrial Fibrillation, Unspecified Used when the provider documents “chronic AFib” but does not specify whether it is persistent, longstanding, or permanent.
I48.21 — Permanent Atrial Fibrillation The heart is in continuous AFib and rhythm control is no longer being pursued. The patient and provider have agreed to manage rate only.
I48.3 — Typical Atrial Flutter Not AFib, but close. Regularly confused by newer coders.
I48.4 — Atypical Atrial Flutter A different electrical pattern from typical flutter.
I48.91 — Unspecified Atrial Fibrillation The catch-all when type is not documented. Also the code most commonly associated with AFib with RVR ICD 10 scenarios when the specific type is not noted.
I48.92 — Unspecified Atrial Flutter
AFib with RVR ICD 10: What You Need to Know
A lot of coders ask specifically about AFib with RVR ICD 10 coding. RVR stands for rapid ventricular response, meaning the ventricles are beating too fast in response to the chaotic atrial signals, usually above 100 beats per minute.
Here is the critical point: RVR is not a separately coded condition. It is included within the AFib code itself. You do not add an extra code for “rapid ventricular response.” Instead, you select the appropriate AFib code based on the documented type.
So if the provider writes “AFib with RVR” but does not specify paroxysmal, persistent, or permanent, you land on I48.91. If they document “paroxysmal AFib with RVR,” you use I48.0.
For billing purposes, AFib with RVR often pushes the encounter toward a higher level of medical complexity. Payers scrutinize these claims carefully because they typically involve ED visits, IV medications, and monitoring. Your documentation must show the heart rate on EKG, the clinical instability, the treatment given, and the patient’s response to therapy. Without those details, even a correctly chosen ICD 10 code for AFib is not enough to protect the claim.
Medical Billing Tips for AFib Unspecified in 2026
Getting paid correctly for AFib claims is getting tougher. Payers have sharpened their review processes, especially for unspecified codes. Here are the most important billing tips to follow right now:
Always query for specificity first. Before defaulting to I48.91, check the chart carefully. If the provider documented any type, use the specific code. If the notes are genuinely vague, query the provider before submitting. A quick clarification can move you from I48.91 to I48.0 or another code, which may affect the DRG and reimbursement.
Document the EKG findings. Claims for AFib, especially AFib with RVR ICD 10, need objective data. The heart rate, rhythm description, and absence of P waves on EKG should all appear in the notes. Payers reject claims where medical necessity is invisible in the record.
Sequence the principal diagnosis correctly. If AFib is the main reason for the encounter, it goes first. If another condition triggered the AFib, that underlying condition leads and AFib follows as a secondary diagnosis.
Add relevant secondary codes. Code the comorbidities. Hypertension, heart failure, sleep apnea, and diabetes all belong in the record when they are present. They affect DRG grouping and tell the full clinical story.
I48.91 falls in MS-DRG v43.0 groups 308, 309, and 310 (cardiac arrhythmia and conduction disorders with MCC, CC, or without). Knowing which DRG you are targeting helps you ensure the documentation supports the severity level.
Do not use I48.9 instead of I48.91. The parent code I48.9 covers unspecified atrial fibrillation AND atrial flutter together. It is non-billable. Always drill down to I48.91 for afib or I48.92 for flutter.
Common Coding Mistakes to Avoid in 2026
These errors come up constantly and they cost money and create audit exposure.
Mistake 1: Using I48.9 instead of I48.91 I48.9 is the parent, non-billable code. The billable version for unspecified afib is I48.91. This is a simple mix-up but it tanks claims.
Mistake 2: Coding RVR as a separate diagnosis RVR is included in the AFib code. Adding a separate code for tachycardia creates a duplicate code situation and draws auditor attention.
Mistake 3: Defaulting to unspecified when specificity exists If the record says “paroxysmal,” use I48.0, not I48.91. Using the unspecified code when documentation supports a specific one is both a compliance issue and a potential revenue problem.
Mistake 4: Ignoring “chronic” AFib documentation When a provider writes “chronic AFib,” many coders still reach for I48.91 out of habit. The correct code in that case is I48.20 (chronic AFib unspecified) unless the type is further specified.
Mistake 5: Failing to code underlying conditions AFib rarely exists in a vacuum. Leaving out hypertension, heart failure, or sleep apnea misrepresents the clinical complexity and leaves reimbursement on the table.
Mistake 6: Submitting without EKG documentation support Payers, especially Medicare, increasingly flag AFib claims without confirmed EKG findings in the chart. No rhythm strip means higher denial risk.
Related ICD-10 Codes to Use Alongside AFib
Depending on what else is going on clinically, these codes frequently pair with the ICD 10 code for AFib:
I10 — Essential (primary) hypertension. One of the most common secondary codes with AFib.
I50 series — Heart failure. AFib and heart failure co-occur frequently. Specific heart failure type (systolic vs diastolic, acute vs chronic) must be documented for the right subcode.
G47.33 — Obstructive sleep apnea. If this is in the record and being managed, code it.
E11 — Type 2 diabetes mellitus. Frequently documented alongside AFib.
Z79.01 — Long-term use of anticoagulants. Most AFib patients are on warfarin, apixaban, rivaroxaban, or similar agents. This code belongs in the record.
Z82.49 — Family history of ischemic heart disease. Relevant for new-onset cases.
2026 ICD-10-CM Updates You Need to Know
The 2026 edition of ICD-10-CM became effective on October 1, 2025. Here is what matters for AFib coding this year:
The core I48.91 code remains active and unchanged in its description. No new AFib-specific codes were introduced in the 2026 update cycle, and no AFib codes were deleted. However, the MS-DRG grouping was updated to v43.0, which affects how claims are bucketed for inpatient reimbursement.
Payers in 2026 have significantly increased scrutiny on unspecified codes across the board, not just AFib. The CMS push toward more specific coding continues, meaning that I48.91 should be a last resort, not a first choice. If the documentation supports a more specific AFib code, you are expected to use it.
Additionally, Risk Adjustment Data Validation (RADV) audits have intensified for Medicare Advantage plans. AFib is one of the highest-volume cardiac diagnoses and therefore one of the highest scrutiny categories. Any discrepancy between the ICD 10 code submitted and what is actually in the medical record is a significant compliance risk heading into 2026.
Electronic health record systems are increasingly deploying AI-assisted coding tools that auto-suggest AFib codes based on clinical notes. While these tools can speed up the workflow, they still require human review. Auto-suggested codes have been flagged in audits when the note language does not clearly support the suggestion.
Frequently Asked Questions (FAQ)
What is the ICD 10 code for AFib unspecified? The correct code is I48.91 — Unspecified Atrial Fibrillation. It is a billable, specific code valid for the 2026 ICD-10-CM fiscal year through September 30, 2026.
What is the PAF ICD 10 code? PAF stands for paroxysmal atrial fibrillation. The ICD 10 code for PAF is I48.0. Use this when the provider documents that AFib episodes come and go on their own and typically last less than 7 days.
What is the AFib with RVR ICD 10 code? There is no standalone RVR code. RVR (rapid ventricular response) is captured within the AFib code. If the type is unspecified, use I48.91. If the type is paroxysmal, use I48.0, and so on.
When should I use I48.91 versus I48.20? Use I48.91 when the provider simply documents “AFib” without any type. Use I48.20 when the provider writes “chronic AFib” but does not add further specifics like persistent or permanent.
Can I48.91 be the principal diagnosis? Yes, absolutely. When AFib (unspecified) is the main reason for the encounter, it should be sequenced as the principal diagnosis. If another condition triggered the AFib, lead with that condition and list AFib as secondary.
Does AFib with RVR require additional documentation beyond the AFib code? Yes. For RVR cases, payers expect documentation of the heart rate (typically 100+ bpm), EKG confirmation, symptoms, the intervention given (such as IV diltiazem or metoprolol), and the patient’s response to treatment.
Is I48.9 a valid billable code in 2026? No. I48.9 is a non-billable parent code. Always use the more specific I48.91 for unspecified AFib or I48.92 for unspecified atrial flutter.
How does atrial fibrillation ICD 10 coding affect DRG assignment? AFib codes group into MS-DRG v43.0 categories 308 (with MCC), 309 (with CC), and 310 (without CC/MCC). Coding comorbidities accurately can move a claim into a higher-paying DRG group.
Final Word: Code Smarter, Not Just Faster
The ICD 10 code for AFib unspecified, I48.91, is one of the most used cardiac codes in the country. And because it gets used so often, it also gets misused often. In 2026, with payers auditing more aggressively and AI tools catching documentation mismatches faster than ever, accuracy is not optional.
The bottom line is straightforward. Always push for specificity in your documentation. Query providers when the record is vague. Code all relevant comorbidities. Make sure RVR encounters include clinical detail that justifies the level of care. And never assume the unspecified code is “safe” just because it is billable.
Coders who understand the full I48 family and know how to apply the atrial fibrillation ICD 10 codes correctly are protecting their organizations’ revenue and their patients’ records at the same time. That is what good coding looks like in 2026.
Last updated: May 2026 | Based on 2026 ICD-10-CM (effective October 1, 2025) and MS-DRG v43.0